What AI Agents for Prior Authorization Mean for Practices Drowning in Administrative Backlog
Table of contents
- Key takeaways
- What Prior Authorization Involves Today
- Where AI Agents Fit in the Prior Authorization Lifecycle
- Intake agent
- Eligibility and requirement discovery agent
- Payer-rules agent
- Medical necessity evidence agent
- Documentation assembly agent
- Submission agent
- Tracking and follow-up agent
- Escalation and appeal agent
- Reference Architecture for AI Prior Authorization Agents
- Data sources
- Integration layer
- Agent orchestration layer
- Governance layer
- Workflow Design: Human-in-the-Loop vs. Full Automation
- Low-risk automation: delegate fully to agents
- Medium-risk automation: agent-drafted, human-confirmed
- High-risk decisions: human judgment, agent support
- KPIs to Measure AI-Agent Performance
- Authorization turnaround time
- First-pass approval rate
- Denial rate
- Staff hours saved
- Key Cost Categories
- Integration costs
- Workflow configuration costs
- Governance and compliance costs
- Ongoing operations costs
- Implementation Roadmap
- Phase 0: Foundation and readiness
- Phase 1: Baseline and prioritization
- Phase 2: Read-only copilot and staff training
- Phase 3: Assisted packet creation and feedback loop
- Phase 4: Submission automation and regulatory validation
- Phase 5: Escalation intelligence
- Phase 6: Continuous optimization and audit
- Risks and Controls
- What AI-Orchestrated Prior Authorization Actually Looks Like
- Conclusion
Prior authorization sits between clinical urgency and administrative friction. It is indispensable to payers, but disruptive for providers and patients. The American Medical Association (AMA) describes it as a cost-control mechanism. It requires advance approval for covered services or medications. An average practice navigates about 39 authorization requests per physician each week. This process consumes roughly 13 hours (close to a day and a half) of physician and staff time. Zoom out from a single practice, and the volume is staggering. Medicare Advantage insurers alone processed nearly 53 million prior authorization requests in 2024, up from 49.8 million the year before.
This unsustainable administrative burden has redirected the industry's focus. Almost 47% of physicians now rank automated administrative systems among their highest investment priorities. The conversation has shifted from debating automation to determining the best way to implement it in practice.
This is where AI prior authorization agents come in — one of the specialized use cases covered in our broader look at AI agents in healthcare. Specifically designed for settings with high authorization volume, fragmented payer workflows, and limited administrative bandwidth, AI agents address challenges for imaging centers, specialty practices, multi-site provider groups, hospitals, and RCM vendors managing multiple accounts. The greatest impact is seen where documentation needs recur, payer rules are clearly defined, and approval delays result in real costs. These situations highlight the exact challenges AI agents were built to solve.
Key takeaways
- Prior authorization is a multi-stage, document-heavy workflow. It consumes roughly 13 hours of physician staff time per week.
- AI agents address the full authorization lifecycle, from intake and eligibility checks to submission, status tracking, and appeals. These are not delivered as a single monolithic tool, but as a coordinated layer of specialized agents.
- Effective deployment requires deliberate architecture, phased rollout, and clear human-in-the-loop boundaries. Organizations that build on solid data foundations and governance controls see compounding efficiency gains.
- Measurable returns include faster turnaround times, higher first-pass approval rates, and reduced manual effort. Strategically, this frees teams to focus on appeals, clinical edge cases, and patient communication rather than repetitive tasks.
What Prior Authorization Involves Today
To appreciate where AI agents can make a difference, it's important to first map the landscape they are entering. Prior authorization is not a single task — it's a multi-stage administrative gauntlet that demands constant coordination between clinical staff, front-office teams, and payer systems, often under tight scheduling pressure and with incomplete information that arrives from multiple directions.
A typical prior authorization workflow spans the following stages:
- Coverage and benefits verification means confirming that the patient's plan is active. It also includes understanding what the policy covers, identifying cost-sharing arrangements, and flagging any plan-level exclusions. These steps happen before a request is ever initiated.
- Authorization requirement determination is the process of determining whether a specific procedure, drug, diagnostic service, care setting, ordering provider, or associated diagnosis triggers a prior authorization requirement. This depends on that payer's current rules.
- Payer policy analysis involves reviewing the payer's clinical guidelines, medical necessity thresholds, mandated documentation checklists, and submission format requirements.
- Clinical documentation assembly means gathering the full body of evidence needed to support the request. This includes notes from the treating, relevant diagnoses, laboratory findings, imaging studies, prescription history, and records of previous interventions. Records of conservative treatment already attempted are also required, as well as the originating order or referral.
- Medical necessity substantiation requires cross-referencing the assembled clinical record against the payer's criteria. Then, an evidence-based argument must be constructed for why the requested service is appropriate for this patient at this point in their care.
- Request preparation and submission means populating the correct payer-specific forms and packaging supporting documentation. The completed request is then transmitted through the payer's required channel. This could be a web portal, a clearinghouse, a direct API connection, a document upload, a fax queue, or phone-based intake.
- Case monitoring and follow-up means tracking open cases across multiple payers and portals. It involves watching for response deadlines and fielding payer requests for supplemental information before an authorization decision is issued.
- Denials management and appeals are necessary when coverage is initially refused. It includes preparing appeal documentation and drafting letters of reconsideration. When clinical judgment is being contested, coordinate peer-to-peer review between the treating physician and the payer's medical director.
Throughout these steps, providers face a substantial documentation burden. For a single prior authorization, they must submit an order or referral, patient demographics, insurance identifiers, and relevant CPT and ICD-10 codes. They must also complete payer-specific intake forms, attach clinical notes, imaging, or laboratory results, prior treatment history, and a letter or Certificate of Medical Necessity, as well as any other attachments required by the service type and plan. Manually gathering, reviewing, and reconciling these records takes significant time. Most providers handle this slowly — only about 40% of authorizations are fully electronic, according to the 2025 CAQH Index. The majority still rely on portals, phone, and fax. Intelligent automation directly addresses and improves this process.
Where AI Agents Fit in the Prior Authorization Lifecycle
Among the AI trends gaining the most traction in enterprise healthcare technology, AI agents stand out because they don't merely surface recommendations for humans to act on; they execute multi-step processes autonomously, hand off context between stages, and escalate to human reviewers only when genuine judgment is required. Examining the full prior authorization lifecycle, each distinct phase aligns naturally with a specialized AI agent, creating a seamless chain in which enriched, structured data flows downstream to the next step.
Intake agent
Every authorization request starts with unstructured or semi-structured information, such as a physician's order or a referral note. The intake agent extracts key variables — procedure, diagnosis codes, providers, payer, care setting, and urgency — and converts them into a structured record. This step prevents errors and missing fields that often disrupt manual workflows early.
Eligibility and requirement discovery agent
Before documentation is gathered or forms are touched, this agent verifies that the coverage picture is accurate and current. It queries payer eligibility systems in real time to confirm active coverage, identify the applicable plan and benefit tier, surface relevant cost-sharing details, and determine whether the requested service actually requires prior authorization under the payer's current rules.
Payer-rules agent
Payer policies are living documents that are regularly revised, making it difficult to track across a large portfolio of contracted plans. Enter the payer-rules agent, which retrieves the most current version of the relevant policy when needed: applicable coverage criteria, medical-necessity thresholds, required submission forms, documentation checklists, and any plan-specific formatting requirements. This ensures every authorization request aligns with the payer's current expectations, directly targeting the leading cause of preventable denials.
Medical necessity evidence agent
Demonstrating medical necessity is central to authorization, and this agent builds the clinical case from the patient's chart. It provides payers with the needed evidence, including diagnoses, disease progression, treatment history, imaging, labs, medications, and specialist notes. Rather than offering raw data, the medical necessity evidence agent organizes evidence by aligning it with payer criteria in a clear summary that strengthens the request.
To stay on the administrative side, the agent surfaces, organizes, and cites existing clinical evidence against payer criteria, automating these manual tasks to increase efficiency. It does not interpret images or render the medical-necessity determination itself. That judgment, and the attestation behind it, remains with a licensed clinician.
Documentation assembly agent
With clinical evidence identified and payer requirements confirmed, the documentation assembly agent’s unique value is its ability to assemble submission-ready packets that are precisely formatted for each payer. It compiles forms and supporting records in the correct sequence, cross-checks against requirements, and clearly itemizes any outstanding elements. This ensures that staff receive a structured, reviewable package with explicit gap alerts, rather than disorganized documents under time pressure.
Submission agent
Payers use a range of submission pathways, from online portals to fax. The submission agent automates this process by selecting the correct channel, confirming transmission, and logging key details. If one method fails, it switches to an alternative, ensuring the request is tracked and auditable throughout.
Tracking and follow-up agent
Most prior authorizations aren't resolved on submission day, making manual status checks time-consuming and inconsistent. The tracking and follow-up agent maintains visibility across open cases, checks payer systems for updates, flags pending and deadline-approaching requests, and alerts staff with needed context for prompt action, replacing reactive efforts with proactive management.
Escalation and appeal agent
When authorizations are denied or pending due to information requests, the escalation and appeal agent’s unique value lies in its disciplined response and rapid routing. It identifies, categorizes, and assigns cases to the proper escalation path, prioritizes urgent cases, and ensures all needed documentation is in place. This approach guarantees prompt, organized action without replacing the human expertise crucial to effective appeals.
Reference Architecture for AI Prior Authorization Agents
Deploying AI agents effectively requires a deliberately engineered stack in which every layer earns its place. The architecture outlined below reflects the kind of purpose-built healthcare AI design that distinguishes production-grade systems from proof-of-concept experiments: modular enough to evolve as payer requirements shift, robust enough to protect PHI at every handoff, and transparent enough to satisfy the compliance obligations that healthcare AI cannot afford to sidestep.
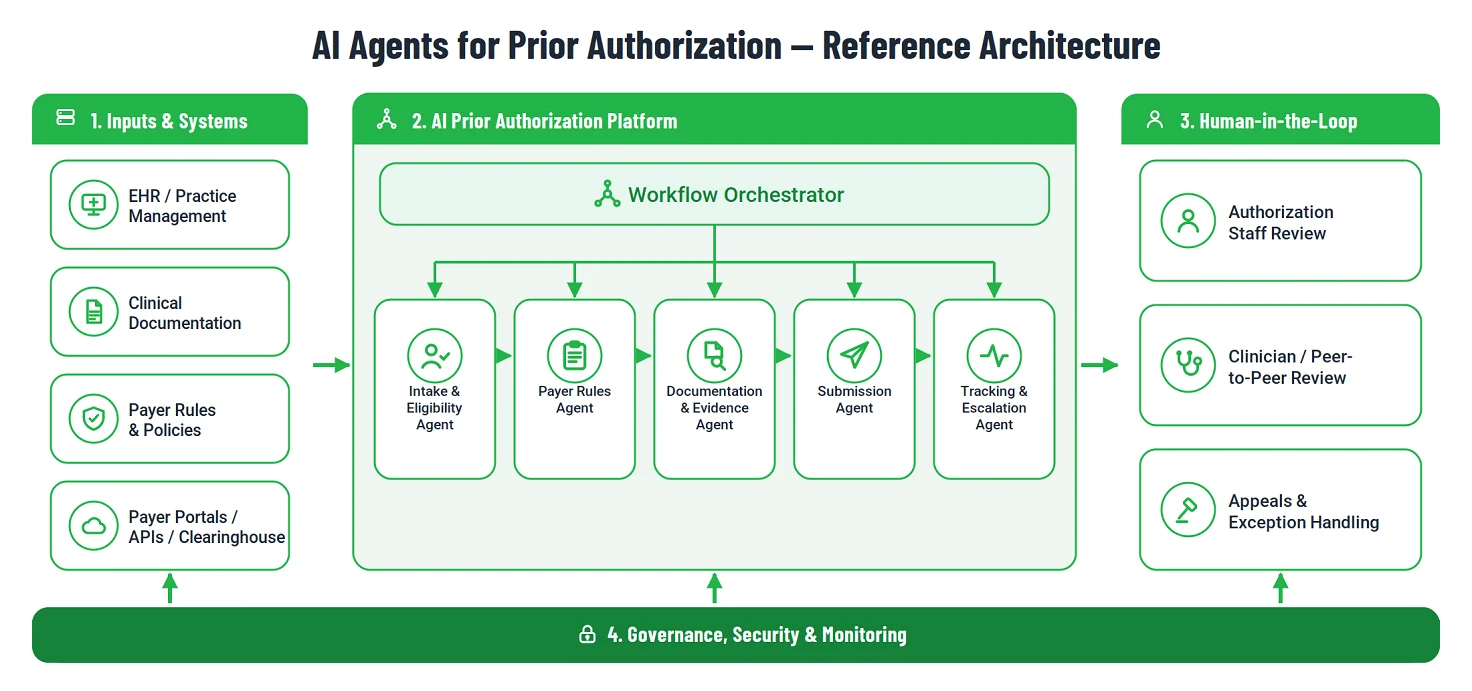
Data sources
This layer collects the information that agents use to build, justify, and submit each authorization request.
- EHR and clinical data — Agents extract structured data: patient demographics, ICD-10, and CPT codes. They also extract unstructured content: physician notes, laboratory results, and imaging protocols, from the electronic health record. This gives downstream agents a complete clinical picture, not a partial one.
- Payer knowledge base — A repository of rules holds current payer policies, medical necessity criteria, and required forms for each plan. Staying current with this knowledge base lets agents catch policy changes rather than generate denials from outdated assumptions.
- External endpoints — Live connections to payer portals, clearinghouses, and government registries allow agents to verify coverage status and authorization requirements in real time. They do not rely on cached data that may no longer reflect the patient's actual plan.
- Historical authorization data — Records of past approvals and denials serve a dual purpose. They train models to recognize patterns in documentation associated with first-pass approval. They also reveal the reasons for recurring denials, payer-specific bottlenecks, and documentation gaps that process improvement efforts can then target directly.
Integration layer
The integration layer manages agent communication with EHR systems, payer platforms, and external registries. The key principle is standards-first, prioritizing APIs and structured data exchange. Portal automation (RPA) is only a fallback when payer APIs are unavailable. Since RPA is rigid — affected by shifting layouts, session expirations, and anti-automation tactics — these paths are closely monitored for silent failures and are temporary solutions until payer APIs are available, not long-term foundations.
- Clinical data standards — HL7 FHIR (R4/R5) provides the protocol for extracting clinical data from EHR systems, while EDI 278 handles pre-authorization transaction transmission to payers, ensuring that data moves in formats that downstream systems are built to receive. Until payer FHIR APIs are widely live, most provider-side submissions still route through portals, clearinghouses, or RPA, which typically includes robust monitoring and alerting to track submission status and exceptions. Therefore, a production system needs both the standards-first path and resilient fallbacks from day one.
- Native EHR embedding — By implementing the SMART on FHIR standard, agents function as native applications within EHR interfaces, preserving patient context and eliminating the context-switching that reduces staff efficiency.
- Transaction security — OAuth 2.0 manages authorization across external connections, while mutual TLS (mTLS) encrypts data in transit. Together, these controls protect the integrity of PHI at every point where agents interact with external payer APIs or third-party systems.
Agent orchestration layer
The orchestration layer runs the operational core. It turns a group of specialized agents into a seamless, end-to-end workflow.
- Workflow orchestrator — Coordinates the sequential and parallel handoffs between agents, from initial intake through final submission, ensuring that outputs from each stage are correctly formatted and available when the next agent needs them.
- Multi-agent coordination — The orchestrator does not route all tasks through a single process. Instead, it distributes work across specialized agents for rules retrieval, evidence collection, and status monitoring. This enables parallel execution and reduces overall turnaround time.
- State management — The orchestrator maintains full context throughout an authorization's lifecycle. If a payer requests supplemental information mid-process, the relevant task is returned to the appropriate agent without discarding the work already completed.
- Human-in-the-loop triggers — When an agent's confidence falls below a set threshold, or when a case involves a clinical judgment call that should not be made by automation, the orchestrator pauses the workflow. It then routes the case to a qualified staff member with the full context attached.
- Retrieval grounding and output verification — Agents generate results using information pulled from source data, not free-form recall. Clinical facts are constructed from records retrieved via FHIR, and a verification step ties each fact to a specific structured source before moving forward. Any claim not linked to a record — such as a treatment or diagnosis without an associated FHIR source — is held back and flagged for human review. This approach makes traceability an active control in the system, not just an audit tool.
Governance layer
The governance layer ensures that healthcare AI meets legitimacy, transparency, and accountability obligations.
- Regulatory alignment — Supports Da Vinci Project profiles, including Coverage Requirements Discovery (CRD), Documentation Templates and Rules (DTR), and Prior Authorization Support (PAS). This positions the system to comply with CMS-0057-F requirements for prior authorization automation. Compliance is becoming a non-negotiable baseline for health system deployments.
These obligations are not aspirational — CMS-0057-F set a phased compliance schedule that is already in motion. As of January 1, 2026, affected payers — Medicare Advantage, Medicaid, and CHIP (both fee-for-service and managed care), and Qualified Health Plans on the federal exchanges — must return prior authorization decisions within 72 hours for expedited requests and seven calendar days for standard ones, with a specific reason attached to every denial. Public reporting of prior authorization metrics began on March 31, 2026. The standardized FHIR Prior Authorization, Provider Access, Patient Access, and Payer-to-Payer APIs must be in production by January 1, 2027. Building agents against the Da Vinci PAS, CRD, and DTR guides now means a system is ready to consume those APIs as payers expose them, rather than retrofitting under deadline pressure.
- Decision traceability — In line with ONC HTI-1 requirements, every agent decision is linked to the specific record or data point in the medical record that informed it. This eliminates the opacity of black-box outputs and provides an auditable rationale for every authorization action the system takes.
- Consent and authorization management — Before the intake agent initiates a workflow, the orchestrator checks the patient's consent and data-use status, enforced through the FHIR Consent resource. While prior authorization generally falls under HIPAA's treatment, payment, and operations provisions, specially protected data — substance use records under 42 CFR Part 2, along with behavioral health, reproductive, genetic, and other categories restricted by state law, and patient-authorized data-sharing flows require explicit checks. The gateway confirms the agent is permitted to access and process each data element and routes restricted cases to staff, rather than proceeding automatically.
- Infrastructure security — The platform works within a BAA-compliant environment that holds SOC 2 Type II or HITRUST certification. An immutable audit trail captures all agent actions and every instance of access to protected health information.
Workflow Design: Human-in-the-Loop vs. Full Automation
Automation ambition in prior authorization must be tempered by clinical and regulatory reality. Not every task in the workflow carries the same consequences if it goes wrong. A well-designed system reflects that asymmetry. It pushes repetitive, low-stakes operations toward full automation, while maintaining human oversight where a mistake could impact patient care, cause compliance issues, or harm payer relationships. The goal is to automate everything that makes sense.

Low-risk automation: delegate fully to agents
Tasks in this tier share a common profile: they are rule-bound, high-volume, and produce straightforward-to-validate outcomes. The unique value of full automation here lies in minimizing human error and freeing staff from routine work. Authorization status checks, case routing based on payer or service type, documentation checklist generation, and eliminating duplicate data entry are all strong candidates for end-to-end agent handling. Because missteps are low-risk and easily corrected, automating these tasks boosts efficiency while protecting against unnecessary costs and delays. This tier maximizes human capacity for more impactful work.
Medium-risk automation: agent-drafted, human-confirmed
This tier covers tasks that agents can handle, but one that needs a human review to provide quality assurance. Assembling draft authorization packets, matching clinical records to payer rules, and identifying missing or weak documentation all fall under this tier. Agents can produce outputs that are mostly complete and well-structured. Yet, they may encounter ambiguous rules or hard cases that benefit from a staff member’s final check. The best approach here is agent-prepared, human-confirmed: fast enough for throughput, careful enough to catch what automation misses.
High-risk decisions: human judgment, agent support
Some decisions in prior authorization are too important or complex for automation. Interpreting medical necessity in unclear cases, choosing a response to a denial, crafting appeals that withstand payer review, and managing urgent escalations all require experienced human judgment. Here, agents support the process by surfacing evidence, flagging key criteria, and ensuring the clinician or appeals specialist can act quickly. The decision itself stays with a qualified human.
Want to understand how AI is reshaping clinical workflows more broadly? Our experts explore the evolving role of intelligent tools in patient-facing and administrative healthcare settings in this in-depth piece on chatbots and ChatGPT in healthcare.
KPIs to Measure AI-Agent Performance
Measuring the impact of AI agents in prior authorization means tracking outcomes, not activity. The metrics below show what matters: faster requests, more first-attempt approvals, and less effort for staff.
Authorization turnaround time
Time elapsed from order placement to final payer decision. Track by:
- Payer and plan type
- Service line and procedure category
- Submission channel and urgency designation
First-pass approval rate
This shows the share of requests approved without rework, extra documentation, or resubmission. It is a good proxy for packet quality and payer-rule matching accuracy. If rates decline, investigate gaps in documentation logic or payer coverage criteria.
Denial rate
This is the percentage of requests that result in a negative payer decision. For clearer insights, break this rate down by:
- Payer and plan
- Service line
- Denial reason code
Looking at the total numbers shows a problem exists, while segmenting the data reveals exactly where it is. For example, in 2024, 7.7% of Medicare Advantage prior authorization requests were fully or partially denied. Given that rates vary widely by payer and program, use this as a Medicare Advantage reference point rather than a universal target. Notably, only about 11.5% of those denials were appealed, yet more than 80% of appeals were overturned. This underscores that low first-pass outcomes are often recoverable—and that disciplined appeals are where measurable value hides.
Staff hours saved
This means less manual effort per authorization in collecting documents, preparing forms, submitting, and following up. The metric is most valuable when compared to a pre-implementation baseline. Ongoing optimization should continue to increase efficiency, not just give a one-time gain.
Key Cost Categories
Deploying AI agents for prior authorization has a cost structure unlike conventional software. The categories below highlight essential investment areas for building a reliable, scalable system. These investments are significant, as the 2024 CAQH Index projects about $20 billion in annual savings from fully automating administrative transactions, with $18.4 billion specific to the medical sector.
Integration costs
Integration costs are the main hurdle when linking agents to their required ecosystem. This includes EHR integration, practice management systems, payer portals, clearinghouses, direct APIs, document repositories, and fax workflows for plans that haven't modernized. These costs are often the most technically demanding and variable part of the initial build. Complexity rises with more payer connections, less mature APIs, and less support for standardized data exchange protocols.
Workflow configuration costs
Before agents can process requests accurately, the underlying logic must be mapped and encoded. Payer-specific rules, service-line authorization requirements, the correct forms for each plan, escalation paths for edge cases, and thresholds that trigger human review all need to be defined. This configuration work is not a one-time effort. As payer policies evolve and new service lines are added, the ruleset needs constant curation to stay accurate and effective.
Governance and compliance costs
Operating in a PHI-adjacent environment entails strict data protection, access controls, audit logging, and HIPAA risk management obligations. These costs cover controls that keep the system trustworthy. These include security architecture reviews, role-based access frameworks, logging agent actions, and versioning mechanisms for traceable rule changes. Skimping here creates regulatory risks that outweigh any short-term savings.
Ongoing operations costs
A prior authorization agent is not a deploy-and-forget system. Sustaining performance requires continuous updates to allow for coverage policies that change, handling exceptions, monitoring models for drift, staff training, and ongoing optimization. Teams that budget for these costs upfront can build systems that improve over time. Those who don't may end up with a solution that slowly deteriorates.
Implementation Roadmap
A prior authorization agent can be introduced as a staff-facing copilot, a background automation layer, a voice-enabled follow-up tool, or a component within a broader RCM transformation. Regardless of the deployment model, most organizations do best when they start narrow. Begin with one service line, a defined payer set, clear human-review checkpoints, and KPIs set before processing the first request. This approach quickly generates value without overreaching into high-risk clinical or payer-facing decisions. Let the system earn trust first.
Phase 0: Foundation and readiness
Execute Business Associate Agreements with AI vendors, perform an SOC 2 or HITRUST security review, and set up role-based access controls before handling patient data. Audit EHR data quality, confirm FHIR/EDI API availability, and designate physician and RCM leaders to oversee implementation and feedback.
Phase 1: Baseline and prioritization
Identify one or two service lines with high authorization volume and consistent documentation needs. Imaging, specialty pharmaceuticals, durable medical equipment, cardiology, oncology, and orthopedics are common starting points. Establish baselines for approval rate, turnaround time, and staff hours before Phase 2.
Phase 2: Read-only copilot and staff training
Start with features that inform: payer-rule lookup, documentation checklist generation, and missing-information detection. Let staff make all decisions while they build trust in agent outputs before the next phase.
Phase 3: Assisted packet creation and feedback loop
Let the agent draft full authorization packets, but require staff review before submission. Use a structured feedback process so every correction improves the system.
Phase 4: Submission automation and regulatory validation
Automate portal and API submissions when payer connectivity is available, and add status polling with deadline-driven follow-up. Integrate payer-specific validation logic to flag cases where state rules, such as gold-card provisions, may make submission unnecessary. Gold-card rules — adopted in a growing number of states — exempt providers who meet a payer's approval threshold (typically 90% or higher) from prior authorization for specific services for 6 to 12 months. Therefore, a submission agent that tracks each provider's gold-card status by payer and plan can skip the workflow entirely when it no longer applies.
Phase 5: Escalation intelligence
Add denial classification, appeal packet drafting, peer-to-peer review routing, and payer-trend analytics. With enough decision history, actionable patterns surface: recurring denial reasons, high-rework service lines, and payer bottlenecks to address in contracts.
Phase 6: Continuous optimization and audit
Regularly track first-pass approval rates and missing-document patterns. Review service-line ROI on a consistent schedule. Conduct quarterly reviews against health equity and transparency standards. Ensure the system stays auditable and defensible as designed.
Risks and Controls
AI agents expedite work and reduce manual effort, but they bring new risks. The table maps key risks to their main controls.
|
Risk |
Example |
Control |
|
Outdated payer rules |
The agent references a superseded policy and assembles documentation around the wrong criteria. |
Keep a versioned payer-rules library with source links, update timestamps, and designated review ownership. |
|
Incomplete documentation |
The request is pending because imaging results or prior treatment records were never attached. |
Run automated missing-document validation against the payer checklist before every submission. |
|
Incorrect medical necessity interpretation |
The agent selects chart evidence that only partially supports the requested service. |
Mandate human review for clinical judgment calls, ambiguous cases, and high-cost procedures. |
|
PHI exposure |
Protected patient data is accessed by an unauthorized user or transmitted through an insufficiently secured channel. |
Enforce role-based access controls, least-privilege permissions, encryption at rest and in transit, and comprehensive audit logging. |
|
Low-confidence automation |
The agent proceeds with submission despite ambiguous or incomplete payer-rule guidance. |
Define confidence thresholds below which cases are automatically routed to staff rather than submitted. |
|
Delayed escalation |
A pending or time-sensitive authorization goes unaddressed until the deadline has passed. |
Implement automated status monitoring, deadline alerting, and prioritized escalation queues. |
|
Portal or integration failure |
A payer portal undergoes a layout change and the submission pipeline breaks silently. |
Monitor transmission success rates, log errors in real time, and maintain tested fallback workflow. |
|
Poor appeal handling |
Denials are contested with boilerplate language rather than case-specific clinical evidence. |
Classify denial reasons at intake and require specialist or clinician sign-off on every appeal packet. |
|
Algorithmic bias |
The model disproportionately generates adverse outcomes for specific demographic or age groups. |
Conduct regular health equity audits and statistical analysis of agent decisions disaggregated by demographic variables. |
|
Lack of explainability |
Clinicians cannot identify which specific chart entry the agent relied on to assert medical necessity. |
Link every agent decision to a direct source record in the EHR, in line with ONC HTI-1 traceability requirements. |
|
Model hallucinations |
The agent fabricates conservative therapy history that does not exist in the patient’s record. |
Require mandatory human-in-the-loop verification for final packet approval, with all clinical facts cross-referenced against structured FHIR data. |
|
Legal and regulatory liability |
An agent makes a determination that qualifies as a medical judgment under SaMD regulations without the appropriate certification. |
Limit agents to organizing and citing evidence, not interpreting images or making determinations; always confirm device/CDS status per deployment (FDA CDS; EU MDR Rule 11). Clinicians own every attestation. |
What AI-Orchestrated Prior Authorization Actually Looks Like
A patient is scheduled for an MRI. The intake agent checks eligibility, confirms that the payer requires prior authorization for the study, retrieves the applicable imaging policy, reviews the chart for conservative therapy records and relevant prior imaging, flags one missing clinical note, assembles the authorization packet, routes it to staff for approval, submits it through the payer's preferred channel, monitors for a decision, and escalates the case if no response is received before the appointment date.
Conclusion
AI agents will not eliminate prior authorization. The administrative and regulatory structures behind coverage decisions are deeply embedded in payer cost management and health system revenue strategies. Instead, AI agents shift what the process requires from staff: simplifying workflows and reducing manual interventions.
The main benefit of agentic automation is reducing repetitive tasks, such as eligibility checks, assembling documents, and tracking delayed cases. This lets staff handle higher-value work, such as interpreting evidence, preparing appeals, and guiding patients.
Organizations will benefit most by maintaining strong data foundations, clear governance, phased deployment, and understanding where it is vital to maintain human input.
If your organization is ready to move from manual queues for insurance authorizations to a smarter, traceable, and continuously improving process, Emerline's team brings the needed technical and healthcare industry experience to build it properly. Reach out to discuss what deploying AI agents would look like for your specific mix of insurance providers, service types, and operational challenges.
Published on Jun 30, 2026





