What a Patient Intake AI Agent Means for the Future of Healthcare Front Desks
Table of contents
- Key takeaways
- What Traditional Patient Intake Actually Costs
- Time losses
- Financial losses
- Clinical impact
- What Is a Medical Patient Intake AI Agent?
- Static/online form
- RPA script
- Rule-based chatbot
- AI intake agent
- How a Patient Intake AI Agent Works: Step-by-Step
- The pre-visit conversation layer
- Data validation and gap detection
- EHR and PMS routing
- Escalation and edge case handling
- Business Impact
- Speed up the check-in process
- Fewer denied claims due to intake errors
- Richer clinical context before the visit
- Patient experience — convenience and shorter wait times
- Governance, Privacy, and Compliance
- What HIPAA actually requires of an intake agent
- The minimum necessary principle, applied to design
- Consent management done correctly
- Audit logging as the line between governed and ungoverned AI
- Human-in-the-loop: defining who reviews what, and when
- Risks and Limitations to Consider
- Risk 1: Incomplete data collection in complex histories
- Risk 2: Misinterpretation of symptoms
- Risk 3: Integration errors with legacy EHR systems
- Risk 4: Erosion of patient trust, without transparency
- Risk 5: Model hallucinations and drift in unstructured data extraction
- Risk 6: Compliance and privacy risks via third-party LLM APIs
- Risk 7: Latency during real-time eligibility checks
- Risk 8: Staff alert fatigue from too many escalations
- Risk 9: Exclusion of patients who can't use the digital intake system
- Who Benefits Most: Best-Fit Organizations
- Multi-location provider groups and large outpatient networks
- Urgent care networks
- Telehealth platforms
- Specialty practices
- How to Evaluate and Deploy a Patient Intake AI Agent
- Step 1: Audit your current intake workflow
- Step 2: Define the scope before you build or buy
- Step 3: Assess your EHR and integration readiness
- Step 4: Pilot, measure, then scale
- Conclusion
In most clinic or hospital waiting rooms, a patient’s first encounter is paperwork. They spend up to 20 minutes filling out repetitive forms before clinical interaction. The cost isn’t just time. A UC San Diego study published in JAMA Surgery found that switching from paper to electronic consent forms reduced entry errors from 32% to 1%. Paper-based intake errors drive billing disputes, compliance gaps, and rework that uses more staff hours. Meanwhile, front-desk teams bear the brunt (transcribing handwriting, chasing missing fields, and answering the same registration questions repeatedly) fueling the burnout behind high administrative turnover.
Patient intake relies on outdated ideas about tolerating unnecessary friction before care. For that exact reason, it’s also where AI agents tend to deliver the fastest value. As the opening interaction in the patient journey, intake is high-volume, highly repetitive, and governed by clear rules — demographic capture, insurance verification, consent collection, intake form completion — which makes it unusually well-suited to intelligent automation. Unlike clinical decision-making, where caution and human oversight must dominate, intake is largely administrative territory: exactly the kind of workflow where an AI agent can operate with meaningful autonomy and produce a fast, measurable return.
This article is part of Emerline's exploration of AI agents in healthcare, examining how purpose-built agents reshape patient and provider experiences. We start here, at the first point of contact.
Key takeaways
- forms have high error rates, which cause financial losses, billing issues, and inefficiencies long after the front desk interaction.
- A patient intake AI agent is an autonomous system with built-in reasoning, validation, and escalation. It adapts its questions, verifies data with live systems, writes structured data to the EHR, and avoids clinical decision-making.
- The business impact extends beyond the front desk. Faster check-ins, fewer intake-related claim denials, and richer pre-visit context all result from capturing clean data early.
- Success depends on governance and disciplined scaling, not just tech. Organizations see results when they define scope, plan for risk, and pilot with clear goals. Those who skip the groundwork struggle with adoption, regardless of the agent's capability.
What Traditional Patient Intake Actually Costs
Before quantifying potential AI recovery, it's essential to pinpoint what traditional intake costs — time, money, and clinical quality. These costs rarely appear in one place, which is why they are often ignored.
Time losses
Time spent on paper-based intake hunched over a clipboard, rewriting insurance details and medical history that almost certainly already exist in the system. Digital intake, even in its more basic forms, compresses that considerably, but the gap widens further with intelligent automation: an AI agent that pre-populates known fields, asks only what's genuinely missing, and validates entries in real time can reduce the same process to a few minutes — time that gets returned to both the patient's day and the clinical schedule.
Financial losses
Every registration carries a real, calculable cost—staff time spent transcribing handwritten forms, correcting illegible entries, and re-keying data across systems that don't talk to each other. That cost compounds downstream: errors introduced at intake (a transposed insurance ID, a misread date of birth, a missing policy number) surface later as claim denials, billing disputes, and the administrative labor required to track down and fix them. What looks like a five-minute front-desk inconvenience often becomes an hours-long billing department problem weeks later.
Clinical impact
Incomplete or inaccurate information gathered before a visit doesn't disappear — it resurfaces in the exam room, where the clinician spends valuable appointment time re-asking questions that should have already been answered, verifying medication lists that were never properly captured, or working from an incomplete history that makes the encounter less efficient and, in some cases, clinically riskier. An appointment that should run on schedule ends up filling administrative gaps the intake failed to close.
What Is a Medical Patient Intake AI Agent?
A medical patient intake AI agent is more than a basic digital form or RPA tool. It operates autonomously, reasoning through conversations, using integrations as needed, and working within guardrails to engage patients in natural language. It is capable of adapting to their responses, validating information in real time, and writing structured data into the EHR. This distinction matters because prior technologies — static forms, RPA, basic chatbots — solve only parts of the problem and fail when intake becomes complex: ambiguous answers, missing fields, or cases outside scripts.
The comparison below makes that progression concrete:
Static/online form
Autonomy: None
Adaptability: None
Integrations: Minimal
What it can and cannot do: Captures structured data according to a fixed script. There is no conditional logic, no real-time validation, and no ability to write data back into the EHR – every submission requires manual staff review before it enters any downstream system.
RPA script
Autonomy: Low
Adaptability: None
Integrations: Partial
What it can and cannot do: Automates the mechanical transfer of data between predetermined systems, such as moving form entries into the EHR. These scripts are rigid by design: any interface change breaks the automation, and anything outside a clean, expected input – unstructured text, missing fields, exceptions – requires human intervention to resolve.
Rule-based chatbot
Autonomy: Low
Adaptability: Low
Integrations: Partial
What it can and cannot do: Rule-based healthcare chatbot walks patients through a predefined decision tree, handling simple, conditional branches, such as “if yes, ask X.” What it cannot do is interpret ambiguous responses, recover gracefully from unexpected input, or adjust to clinical nuance. Once a conversation departs from its scripted path, the chatbot fails.
AI intake agent
Autonomy: Medium
Adaptability: High
Integrations: Full
What it can and cannot do: Understands natural language, adapts its line of questioning based on patient responses, detects gaps and inconsistencies as they occur, and writes structured data directly into the EHR or practice management system via HL7 v2 or FHIR. Edge cases are escalated to staff rather than assumed or guessed. Critically, it does not render clinical decisions or interpret symptoms diagnostically – its domain is administrative, not medical.
One point deserves emphasis. A patient intake AI agent does not diagnose or make clinical decisions. It doesn't interpret symptoms medically, and it isn't designed to do so. This boundary isn't a flaw — it intentionally keeps the agent focused on administrative tasks, making it trustworthy for organizations and comfortable for patients.
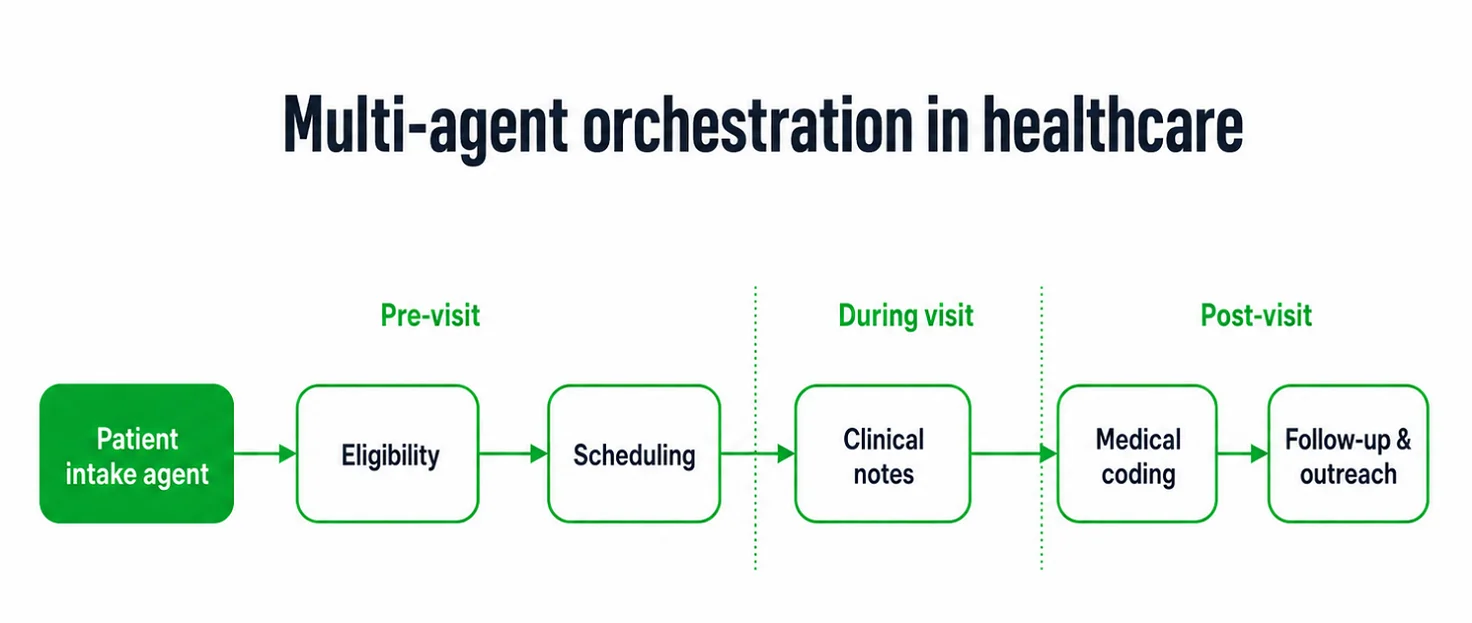
Positioned correctly, the intake agent isn't an isolated tool—it's the first node in a much longer chain. The data it collects and structures at the very first point of contact flows downstream into eligibility verification, scheduling, clinical documentation, medical coding, and follow-up outreach, with each subsequent step benefiting from the accuracy established at intake. This kind of sequential handoff between specialized agents is the foundation of effective multi-agent orchestration in healthcare, where the value of automating any single step compounds as it propagates through subsequent stages.
How a Patient Intake AI Agent Works: Step-by-Step
The instinct to see an AI intake agent as a polished form overlooks what actually happens beneath the surface. A form asks the same questions to every patient, regardless of their answers. An agent, by contrast, listens, adjusts its questions in real time, checks information against live systems, and decides the next step — all before staff gets involved. This is how the process works in practice.
The pre-visit conversation layer
The agent contacts the patient before their clinic visit (usually 24 to 48 hours before the appointment) via SMS, email, patient portal, or app, depending on the organization. During this conversation, it gathers:
- Demographics: name, date of birth, address, preferred language
- Insurance details: payer, policy number, group ID, guarantor information
- Consent and authorizations: treatment consent, HIPAA acknowledgment, release of information
- Chief complaint and symptoms: reason for visit, onset, severity, relevant history
- Current medications and allergies: including over-the-counter drugs and supplements
- Referral information: referring provider, reason, prior records to retrieve
- Pre-visit questions: anything the patient wants raised with the clinician
Adaptive flow sets this apart from static forms. A patient mentioning chest pain triggers immediate follow-up on duration and radiation; a patient without medications sees the allergy section shortened. The conversation adapts to responses instead of following a preset script.
Data validation and gap detection
Gathering information is only half the job — the agent also checks the data quality before sending it to the care team.
- Insurance eligibility is checked in real time: The agent queries the payer during the conversation, not on the morning of the appointment, leaving time to correct problems. If coverage has lapsed or the policy number is wrong, the patient is notified, and the staff is flagged immediately.
- Missing fields are caught before the appointment: Rather than arriving at check-in with an incomplete record, the agent prompts the patient to fill the gap directly or routes a task to staff when human follow-up is warranted.
- Contradictory or unclear answers are handled smoothly: An unknown medication or a conflicting birthdate prompts a clarifying question instead of being logged as is. Anything unresolved is flagged for staff review before the visit.
By the time the appointment begins, the record on file is complete, verified, and internally consistent.
EHR and PMS routing
After validation, the agent formats and routes data to clinical systems via HL7 v2 or FHIR, the standard for major EHR platforms. Importantly, the agent does not enter information into the provider-authored clinician note. It fills patient-supplied fields: demographics into registration, insurance into eligibility, and chief complaint, symptoms, medications, and allergies into intake and questionnaire sections. Medications and allergies are marked as patient-reported and sent for clinician reconciliation, not merged into the active record.
This routing matters; misformatted data or manual re-keying from PDFs often causes transcription errors and delays. Integrated properly, the clinician sees a pre-visit summary — reason for visit, flagged symptoms, patient-reported medications for reconciliation, insurance status, and patient questions — allowing appointments to start with care, not data entry.
Escalation and edge case handling
A well-designed agent cannot resolve everything on their own, and intake conversations can break down. Escalation is triggered by:
- A deterministic match against a set list of safety keywords (such as "chest pain," "trouble breathing," or "sudden weakness"). This check uses fixed terms and operates independently of the language model, not interpreting the patient's condition.
- Patients who indicate a need for an interpreter or show signs of limited health literacy
- Insurance scenarios complex enough to require staff judgment
- Consent or legal situations that fall outside standard workflows
- Record conflicts that clarifying questions alone cannot resolve
This distinction is deliberate and carries regulatory weight. The agent does not assess symptom severity, assign acuity, or advise the patient on their symptoms—doing so could reclassify the software from administrative tooling to a regulated medical device under the FDA's Clinical Decision Support framework or EU Medical Device Regulation.
Because the agent is patient-facing, it is especially easy to cross that line with time-critical determinations. Therefore, when a safety keyword matches, the agent does exactly two things. First, it surfaces standard, non-individualized guidance (e.g., prompting every patient to call emergency services if they believe they are experiencing an emergency). Second, it routes the conversation to a qualified human. Clinical judgment remains entirely with the person.
When these occur, the agent halts automation, notifies the right staff, and records gathered information — the handoff is documented, so staff have full context.
Incomplete intakes receive proactive treatment. If a patient starts (but does not finish) the agent sends a reminder; if the intake remains incomplete before the appointment, the front desk is notified. The appointment proceeds as scheduled, with the incomplete intake flagged for the care team to resolve at check-in.
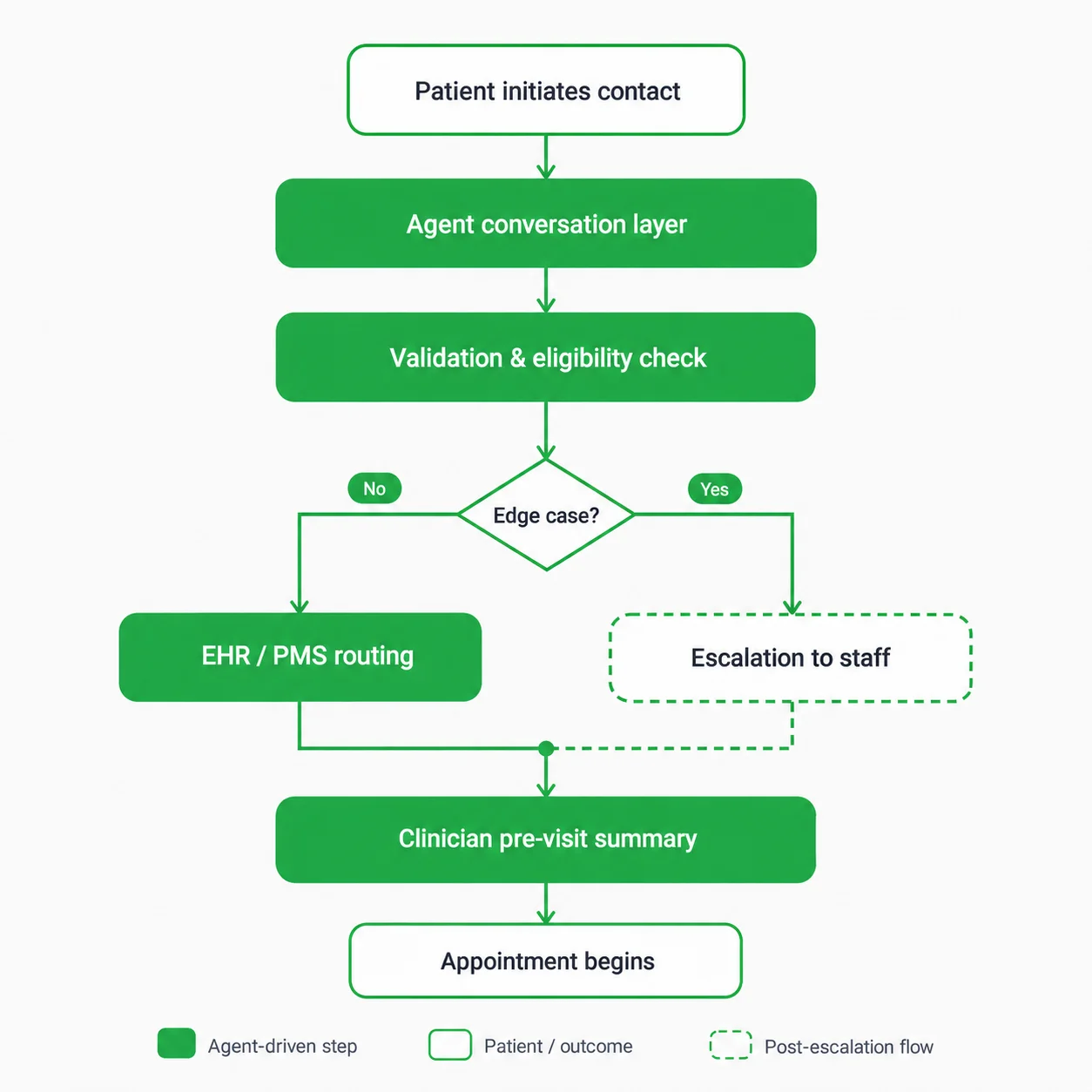
The diagram below traces this entire sequence, from the patient's first point of contact through escalation paths to the clinician's pre-visit summary.
Business Impact
The operational case for a patient intake AI agent is clear: improving accuracy and efficiency early in the patient journey reduces delays, errors, and costs. These benefits address issues that would otherwise interrupt care, increase expenses, or impact patient satisfaction.
Speed up the check-in process
By completing and validating intake before arrival, patients can transition more quickly from the waiting room to the exam room. This reduces wait times and ensures that front-desk staff can focus on assisting those who truly need help, rather than on administrative tasks. The scale of the opportunity is huge: the CAQH 2024 Index estimates that fully automating administrative workflows — including intake and eligibility on the front end—could save providers and staff roughly 70 minutes per patient visit, time currently lost to phone calls, manual verification, and re-keying data.
Fewer denied claims due to intake errors
Denials cluster at the point where data first enters the system. In Experian Health's State of Claims 2025 provider survey, inaccurate or incomplete information captured at check-in ranked third among the most common causes of denials, and more than a quarter of providers reported that at least 10% of their denials trace back to intake errors. The same survey found that 50% of providers now name missing or inaccurate claim data as the top driver of rising denial rates. Catching an incorrect policy number or a demographic mismatch at intake — rather than after submission — prevents the rejection, rework, and delayed payment that follow, improving cash flow and reducing administrative load later in the cycle.
Richer clinical context before the visit
When clinicians receive a complete summary in advance, they can immediately focus on diagnosis and care, leading to more efficient, higher-quality patient interactions.
Patient experience — convenience and shorter wait times
Home-based digital intake allows patients to complete forms comfortably and avoid redundant questions, leading to shorter wait times and the sense that their provider is well-prepared for their visit and can provide better care.
Governance, Privacy, and Compliance
Patient intake is the entry point to care and the first place protected health information enters the system. Strong governance from the outset enables secure, efficient patient onboarding — it's not an afterthought added post-deployment.
What HIPAA actually requires of an intake agent
Once a patient intake AI agent processes, transmits, or stores PHI for a covered entity, it becomes a HIPAA business associate with specific, non-negotiable obligations. The agent must operate in an environment designed for:
- Encryption in transit and at rest: PHI exchanged among the patient, agent, and other systems is protected with current protocols: TLS 1.3 in motion (with TLS 1.2 as the minimum fallback for legacy payer and clearinghouse endpoints), and AES-256 at rest.
- Access controls: Role-based permissions specify who can access patient data, ensuring only authorized personnel or systems can view it.
- Audit trails: Every action involving PHI is logged with a timestamp, user or system identity, and action type.
- Breach notification readiness: If PHI is exposed, the organization must reconstruct exactly what was accessed, when, and by whom—a task that requires structured, comprehensive logging.
A signed Business Associate Agreement between the healthcare organization and the AI vendor is required before any PHI is entered into the system — not a formality to be finalized later.
The minimum necessary principle, applied to design
HIPAA's minimum necessary standard limits data collection, access, and sharing to only what each function needs, helping intake agents reduce risk by ensuring they access only essential information. This means:
- The agent doesn't collect diagnostic history; there's no reason to gather it for a routine visit.
- Raw conversation transcripts aren't kept longer than operationally necessary.
- Fields aren't passed to systems that don't need them.
Define and limit what an agent collects before deployment, not based on the hope that 'more data might be useful.' Each field should serve a specific downstream purpose.
Consent management done correctly
Because the agent is often the first system a patient uses before a visit, it's the natural point to capture consent if handled carefully. This efficient capture at the initial touchpoint streamlines compliance, builds trust, and reduces administrative burden. A well-governed agent presents consent language clearly and records explicit acknowledgment with a timestamp and session ID. This applies across several categories:
- Treatment consent: authorization for the upcoming visit
- HIPAA Notice of Privacy Practices: acknowledgment that the patient has received the organization's privacy notice
- Communication preferences: opt-in or opt-out status for SMS and email outreach
- Release of information: where applicable, authorization to share records with referring providers or other third parties
Store consent records separately from general data, link them to the patient's permanent EHR record, and make them retrievable for audits.
Audit logging as the line between governed and ungoverned AI
Auditability distinguishes governed deployments from those that only appear functional. Every intake agent action should log:
- When a conversation started and ended
- Which data fields were collected, and when
- Whether the patient completed the intake or abandoned it partway through
- What validation checks ran, and what they returned
- Whether escalation was triggered, and for what reason
- When and how data was written to the EHR or PMS
- Which staff member reviewed any flagged records, and when
These logs serve three purposes: supporting compliance investigations, enabling operational debugging, and informing continuous improvement based on agent performance. Logs should be tamper-evident, retained as required (HIPAA mandates at least six years for some records), and directly accessible to compliance staff — engineering help shouldn't be needed to retrieve them.
Human-in-the-loop: defining who reviews what, and when
Automation doesn't eliminate supervision. Responsible deployment defines review checkpoints where human judgment remains in the workflow, including:
- Flagged or incomplete records: any intake the agent can't complete or that triggers an exception appears in a staff queue before the appointment, not after.
- First-pass insurance exceptions: unclear or negative eligibility results are reviewed by billing or front-desk staff before the patient arrives.
- Escalated conversations: cases that leave the automated flow require staff follow-up and documentation.
- Periodic performance review: someone in the organization monitors aggregate intake metrics (rates, frequency, errors) to catch systemic issues early.
The goal isn't to review everything, which would defeat automation. It's to identify where human judgment adds value and ensure qualified people are present at those points.
Risks and Limitations to Consider
No intake agent deployment is risk-free, but proactively identifying and addressing risks protects clinical outcomes, patient trust, and compliance. Planning ahead ensures the benefits of automation do not erode over time.
Risk 1: Incomplete data collection in complex histories
The agent may miss important clinical details when a patient's history is complex or spans multiple providers, and won't always know what it missed.
Risk 2: Misinterpretation of symptoms
Natural language descriptions of symptoms are often ambiguous. An agent structuring them without clinical judgment risks adding inaccuracies to the EHR and affecting care decisions.
Risk 3: Integration errors with legacy EHR systems
Older EHR platforms weren't built for real-time API communication, and a poorly mapped integration can silently corrupt field values, create duplicate records, or drop data entirely, often without triggering any visible error.
Risk 4: Erosion of patient trust, without transparency
Patients who are not sure why an automated system requests medical data may disengage, answer incompletely, or lose confidence — undermining the improvements the agent aims to provide.
Risk 5: Model hallucinations and drift in unstructured data extraction
Large language models are probabilistic. An agent without strict guardrails or semantic checks can create medical term errors or misinterpret typos — leading to changes in medication, dosage, or allergies. To systematically manage model hallucinations and data drift, the deployment should follow the NIST AI Risk Management Framework. In practice, this means implementing continuous regression testing, setting up semantic validation guardrails, and enforcing 'Zero Data Retention' policies with third-party LLM APIs so that PHI is never used to train foundational models.
Risk 6: Compliance and privacy risks via third-party LLM APIs
Sending PHI through generative AI APIs exposes the organization to regulatory risk. Without Zero Data Retention or a fully executed BAA for each LLM sub-processor, organizations risk major HIPAA violations and data leaks.
Risk 7: Latency during real-time eligibility checks
Live queries to insurance clearinghouses or payers can cause 10-15 second API delays. If the interface doesn't manage the wait (using micro-engagement cues, for example) patients may think the system froze and abandon digital intake, forcing manual check-in.
Risk 8: Staff alert fatigue from too many escalations
Overly broad escalation criteria inundate teams with low-priority exceptions, leading to alert fatigue and staff bypassing automated workflows in favor of paper-based processes.
Risk 9: Exclusion of patients who can't use the digital intake system
A digital-only intake process risks marginalizing the patients who need support most — older adults, individuals with low digital literacy, and patients with limited English proficiency. Beyond equity, this creates severe legal liabilities under Section 1557 of the ACA and the ADA, which strictly mandate meaningful access and language assistance. Failing to provide a non-digital alternative or language support can lead to regulatory investigations, substantial fines, and other federal enforcement actions for non-compliance.
Who Benefits Most: Best-Fit Organizations
While a patient intake AI agent adds value in nearly any healthcare setting, some organizations see returns faster and more clearly — usually because their intake issues are more pronounced, patient volumes are higher, or they have fewer pre-visit touchpoints.
Multi-location provider groups and large outpatient networks
Organizations with many sites often face intake inconsistency — different front-desk teams, varying processes, and no unified performance view. An AI agent standardizes experience and data quality across the system while giving leadership a single set of metrics rather than inconsistent anecdotes.
Urgent care networks
Speed defines urgent care, and friction at intake undermines it. High, unpredictable patient volume and the need to move people quickly from waiting to exam rooms make this a strong fit — every minute saved at intake compounds across daily visits.
Telehealth platforms
In virtual care, intake often matters more than in a physical clinic, since it may be the only pre-visit touchpoint before the clinician appears. Without a front desk to catch errors, a well-designed agent becomes essential for telehealth organizations to deliver a complete clinical picture the moment a virtual visit begins.
Specialty practices
Cardiology, oncology, orthopedics, and similar fields require pre-visit data beyond basics — prior treatment history, relevant imaging, and medication regimens. An agent that adapts questioning to the specialty, instead of a generic script, collects exactly the information specialists need.
Across all four profiles, a common thread emerges: the more intake volume, complexity, or pre-visit separation there is, the more friction it creates. An AI agent can significantly shift the equation.
How to Evaluate and Deploy a Patient Intake AI Agent
Deploying an AI intake agent is not just a software purchase — it’s an operational change that affects patients, clinicians, billing staff, and IT. Organizations that see it as procurement struggle to adopt it; those that treat it as a cross-functional initiative succeed.
The four steps below are not a vendor checklist; they are the internal groundwork to complete before, during, and after involving a vendor.
Step 1: Audit your current intake workflow
Before evaluating technology, map your actual process — not just what’s in official documentation. The two seldom match as closely as expected.
Document the following:
- Every touchpoint between a patient being scheduled and their record being ready for the clinician, including who handles each step and in which system.
- Record duplicate data entry, such as patients completing paper forms that staff later re-enter into the EHR, a pattern that is almost never on official process maps.
- Average intake completion time, segmented by new versus returning patients and by appointment type.
- The error rate in demographic and insurance data, drawing on denial reports as a direct measure of how often intake mistakes translate into rejected claims.
- Weekly staff hours consumed by intake-related tasks: data entry, verification calls, chasing incomplete forms, correcting errors before appointments occur.
While documenting, note steps that exist solely due to obsolete systems, handoffs with lost or duplicated information, and staff improvisation where processes no longer reflect reality. This audit identifies where an agent has the most impact and provides baseline figures to demonstrate ROI once the AI agent is live.
Step 2: Define the scope before you build or buy
The most common deployment mistake is leaving the agent's boundaries undefined. When nobody explicitly decides what the agent handles and what it doesn't, staff fill that vacuum with assumptions — and those assumptions are rarely consistent across a team.
The scope should be defined across four dimensions:
- Patient population: Which patients go through the automated flow? New patients only, or returning patients, as well? Should patients with complex chronic conditions be included from the start, or only straightforward visit types?
- Appointment types: Pre-operative intake for surgical patients requires different data than routine follow-ups. Specify which appointment types are in the initial deployment.
- Data fields: List the precise fields the agent will collect. Instead of "insurance information," specify "subscriber name, member ID, group number, payer name, and primary versus secondary coverage."
- Escalation criteria: Document exactly when the agent stops and hands off to a human, including clinical, administrative, and patient experience flags.
Equally important is documenting what staff will continue handling by design, not default. This reassures staff and protects the agent from blame for out-of-scope gaps.
Step 3: Assess your EHR and integration readiness
Most organizations underestimate this step, which often delays or derails deployment. Integration complexity is a shared issue; your organization’s readiness must be clear before signing contracts.
Questions worth answering internally before engaging vendors:
- Which EHR or PMS does intake data need to reach, and which version is currently running?
- Does the EHR support HL7 FHIR R4 APIs natively? If not, is a middleware layer already in place, or does one need to be built?
- Who within IT owns EHR integrations, and what capacity do they currently have available?
- Is patient identification handled through a consistent Master Patient Index, or are duplicate records a known, unresolved issue?
- What change management policies govern EHR configuration changes? Some organizations require months of internal approval before any field mapping can be modified.
Treat these as warning signs with vendors: inability to name EHR platforms they have live integrations with, no documented field mapping, no sandbox for pre-launch testing, or go-live timelines that skip parallel intake runs.
Strong integration readiness means your IT team can state which API endpoints are used, how each field maps to the EHR, and what the rollback plan is if problems arise after go-live.
Step 4: Pilot, measure, then scale
A pilot is only useful if success is defined beforehand. “We’ll see how it goes” is an uncontrolled experiment with no exit criteria.
When choosing a pilot segment, start where the agent is likely to succeed and where mistakes have low risk — usually a single location, one standardized appointment type, and digitally comfortable patients.
From day one, track the following metrics:
|
Metric |
What it tells you |
|
Intake completion rate |
The proportion of patients who finish the agent-led process without abandoning it partway through. |
|
Time to complete intake |
Whether the agent is genuinely faster than your established baseline. |
|
Data accuracy rate |
How frequently agent-collected information requires manual correction before the appointment. |
|
Insurance verification straight-through rate |
How often eligibility is confirmed automatically versus requiring staff follow-up. |
|
Escalation rate |
How often the agent hands off to staff – too high suggests scope issues, too low may mean it’s failing to escalate when it should. |
|
Denied claims linked to intake errors |
The ultimate downstream measure of whether intake quality is actually improving. |
Define what counts as "ready to scale" before launching the pilot. For reference: if completion rates top 80%, data accuracy exceeds 95%, and intake-related claim denials fall at least 30%, expansion is reasonable. Falling short isn’t failure — it’s a diagnostic. Address specific gaps before expanding, not by abandoning the initiative.
Scale incrementally — one location or appointment type at a time, with each expansion a mini-pilot measured the same way as the first. Scaling too quickly often reveals issues; the discipline used in the pilot should guide every phase.
Conclusion
It's worth returning to the distinction made earlier in this article, because it's the one that separates organizations that see clear improvements in efficiency and data quality from those left disappointed by intake automation: a patient intake AI agent is not a faster form, and it is not a chatbot wearing a clinical costume. It is the managed delegation of the very first operational step in a patient's journey — handled with the reasoning, validation, and governance that step actually requires, and handed back to staff at precisely the moments where human judgment matters more than automation ever should.
This distinction makes intake an ideal starting point for a broader AI agent strategy. Returns are quick and measurable; risks are administrative, not clinical; and data quality here strengthens all downstream processes that depend on accurate initiation.
Building such an agent — one that integrates with legacy EHRs, meets HIPAA requirements, and knows when to transfer cases to humans — is not a weekend project, nor is it suited for generic chatbot vendors. It needs healthcare engineering experience, real knowledge of clinical workflows, and a deployment philosophy focused on incremental trust.
That’s the work Emerline does. If you want to move past paper forms and disconnected systems to a faster, more accurate, trustworthy intake process, reach out to Emerline's team to discuss what a properly architected patient intake AI agent would look like for your organization's specific EHR environment, patient population, and operational priorities.
Published on Jun 26, 2026





