AI Agents for Revenue Cycle Management in Healthcare: A Practical Guide for Providers
Table of contents
- Key takeaways
- Why the Revenue Cycle Leaks Money
- Most denials are born at the front end
- Reactive denial management costs more — and often recovers nothing
- The leak doesn't end with the payer
- What Is an AI Agent for Revenue Cycle Management?
- Agent vs. RPA bot vs. point solution
- What an agent doesn't do
- How It Works: An Agent at Every Stage of the Cycle
- Eligibility and benefits verification
- Prior authorization
- Medical coding and charge capture
- Claim scrubbing and submission
- Denial management and appeals
- Patient billing and collections
- Under the hood
- Integrating RCM Agents with Your Systems
- Connecting the agent
- FHIR is the future; X12 is the present
- Patient matching and PHI boundaries
- Fitting into the billing team's workflow
- Ready-Made Platforms vs. Custom Development
- What the platforms cover well
- Where custom earns its place
- Compliance, Safety, and Trust
- The basics, applied to money and PHI
- Coding is where the human sign-off isn't optional
- Payer-side AI is already drawing fire
- Regulation as tailwind, not just constraint
- The honest caveat on autonomy
- Metrics and ROI
- What to measure
- A worked example
- The AI cost paradox
- Set honest expectations
- Implementation Roadmap
- Conclusion
- Frequently Asked Questions
- How do AI agents reduce claim denials?
- Which RCM tasks can actually be automated?
- Does an RCM agent integrate with Epic, athenahealth, or other systems?
- Is AI-driven prior authorization compliant with CMS rules?
- Will an RCM agent replace our billing staff?
- How much does an RCM agent cost?
- What's a realistic denial-reduction target?
Every year, the gap between what providers earn and what they actually collect gets wider. In 2025, the more than 2,300 hospitals tracked by Kodiak Solutions lost over $48 billion in net revenue to denials and uncollected patient balances — a 25% jump from $38.6 billion the year before. The increase was driven almost entirely by clinical denials: claims rejected for missing prior authorizations or medical necessity.
What makes this so costly isn't just the denials themselves — it's what happens after. Reworking a denied claim is expensive and slow, so a large share of denials are simply written off. AHIMA's estimates that 35-60% of denied claims are never resubmitted at all. That's not delayed revenue — it's revenue gone for good, lost to administrative friction rather than any real coverage dispute.
This is exactly the kind of work AI agents in healthcare are built for: high-volume, rule-driven, repetitive financial tasks that span the entire revenue cycle, from eligibility checks to denial appeals. But (and this is where this guide differs from most) an AI agent only moves these numbers when it's integrated properly and measured honestly. The rest of this article walks through where revenue actually leaks, what an RCM agent does at each stage of the cycle, how to integrate it, and how to tell whether it's working.
Key takeaways
- The revenue cycle leaks at both ends — payer denials at the front, uncollected patient balances at the back. Most of those losses are administrative, not clinical, which is exactly what makes them automatable.
- Most denials are born before the claim is ever submitted, with registration and eligibility errors being the single largest source. So, the cheapest place to stop a denial is the front desk, not the appeals queue.
- The real leverage is orchestration, not point solutions. An agent that owns several stages of the cycle end to end is more effective than individuals making decisions along the way.
- Faster isn't automatically cheaper. Measure net effect — savings minus the fully loaded cost of the AI and any transaction volume it adds — not just the speed-up on a single task.
- A realistic planning target is a 30-40% reduction in denials where the evidence is strongest (front-end and scrubbing); build the business case on that, not on vendor headline numbers.
Why the Revenue Cycle Leaks Money
It's tempting to think of denials as a billing-department problem — something that happens at the end, when a claim has been rejected. In reality, the revenue cycle leaks at every stage, and most of the leaks begin long before a claim is ever submitted. Money is lost across a chain: eligibility errors at check-in, delays and missing prior authorizations, coding mistakes, rejected claims, and unpaid patient balances. Understanding where the money actually disappears in that chain is what tells you where an agent earns its keep.
Most denials are born at the front end
The single largest source of denials isn't bad luck at adjudication. It's bad data at registration. Front-end issues like wrong insurance details, inactive coverage, and missing prior authorizations have consistently accounted for roughly half of all denials, with registration and eligibility alone the top cause for years. The problem is that these errors are invisible when they happen. A coverage mistake made at check-in doesn't surface until the claim bounces back weeks later. At this point, a clean claim has become a denied one, and a five-second fix has become a multi-step appeal. The cheapest place to stop a denial is the front desk, not the appeals queue.
Reactive denial management costs more — and often recovers nothing
Once a claim is denied, the economics turn against the provider. Reworking a single denied claim costs $25 for a practice and up to $181 for a hospital (AHIMA) — and an appeal can take weeks to resolve. For smaller-dollar claims, staff often conclude it simply isn't worth the effort, which is why 35-60% of denied claims are never resubmitted at all. That figure should reframe how you think about denials: a large share of denied revenue is never recovered, not because the claim was wrong, but because chasing it costs more than it's worth. Every dollar prevented up front is far cheaper than the same dollar fought for on the back end, and many of those back-end dollars are gone for good.
The leak doesn't end with the payer
The final stretch of the cycle is now one of the fastest-growing holes. As high-deductible plans push more of the cost onto patients, a rising share of revenue depends on collecting directly from people after care is delivered, and providers are collecting less of it. Kodiak's data show the patient share of net revenue rising even as the collection rate on that share fell from 45% to 42% in a single year. A modern revenue cycle leaks at both ends: payer denials on one side, uncollected patient responsibility on the other. An honest view of where the money goes has to account for both.
Before turning to the solution, it helps to see the whole cycle at a glance — where each stage leaks money, and why manual workflows can't keep up.
|
Stage |
Where the money leaks |
Why the manual process fails |
|
Eligibility & benefits |
Coverage checked wrong or not at all, so the claim is doomed before the visit |
Staff verify manually against multiple payer portals; under time pressure, checks get skipped or rushed |
|
Prior authorization |
Care delayed or delivered without auth, then denied for medical necessity |
Gathering clinical evidence and chasing payers is slow, and requirements change constantly |
|
Medical coding |
Under-coding leaves revenue on the table; over-coding triggers denials and audit risk |
Coders work from dense documentation by hand; volume forces speed-vs-accuracy tradeoffs |
|
Claim scrubbing & submission |
Errors slip through and become denials instead of being caught pre-submission |
Payer-specific edit rules are too numerous, and they change too often to check manually |
|
Denial management |
A large share of denials are never reworked; they are written off as permanent loss |
Appeals are labor-intensive, so low-dollar claims aren't worth chasing |
|
Patient collections |
A growing patient-responsibility share goes uncollected after the visit |
Manual statements and calls are slow, generic, and easy for patients to ignore |
What Is an AI Agent for Revenue Cycle Management?
An AI agent for revenue cycle management is software that autonomously carries out the financial and administrative work of the revenue cycle — verifying insurance eligibility, preparing and submitting prior authorizations, validating codes, scrubbing and tracking claims, and drafting appeals. These tasks are performed while plugged directly into the EHR, practice management system, and payer systems it needs to act on. The key word is autonomously: instead of flagging work for a person to pick up (the way most medical billing software does) the agent reasons through the task, does it, and pulls in a human only when something genuinely needs judgment.
That autonomy is what sets an agent apart from the automation most billing teams already run.
Agent vs. RPA bot vs. point solution
Almost everything in RCM gets marketed as "automation," so it's worth being precise about what you're actually evaluating.
A robotic process automation (RPA) bot follows fixed scripts. If a screen looks a certain way, it clicks in a certain place. That works well for stable, repetitive steps, but it falters the moment a payer redesigns a form or when an unusual case shows up — and unusual cases are the norm in billing, not the exception.
A point-solution AI is smarter within a narrow lane. It might predict which claims are likely to be denied, or read a document and pull out the right codes, then hand the result back to staff to act on. This is useful, but it covers only one link in the chain — and it stops there.
An orchestrated agent works across links. It can confirm a patient's eligibility, recognize that a procedure needs prior authorization, pull the clinical documentation to support it, submit the request, and track it to a decision — looping in a person only where the judgment call is real. Your investment isn't just a better algorithm. It's the removal of all the manual handoffs between steps that used to require their own tool and their own person.
Most of the market hasn't gotten there. What gets sold as "AI for RCM" is still mostly point solutions: a denial predictor from one vendor, an eligibility checker from another. Each is fine on its own, but staff is left to stitch the gaps between them by hand. The payoff from orchestration is exactly those gaps — an agent that owns a whole stretch of the cycle, so the handoffs that quietly cost time and money stop being manual.
What an agent doesn't do
An RCM agent runs the administrative and financial machinery of the cycle. It does not practice medicine. It won't decide whether a service is medically necessary, it won't diagnose, and it won't second-guess a clinician. Its job on something like prior authorization, for example, is to assemble the evidence — find the relevant notes, map them to the payer's criteria, and lay it all out — so a clinician or the payer can reach a decision faster — and with a complete record. It builds the case and leaves the final decision to a person.
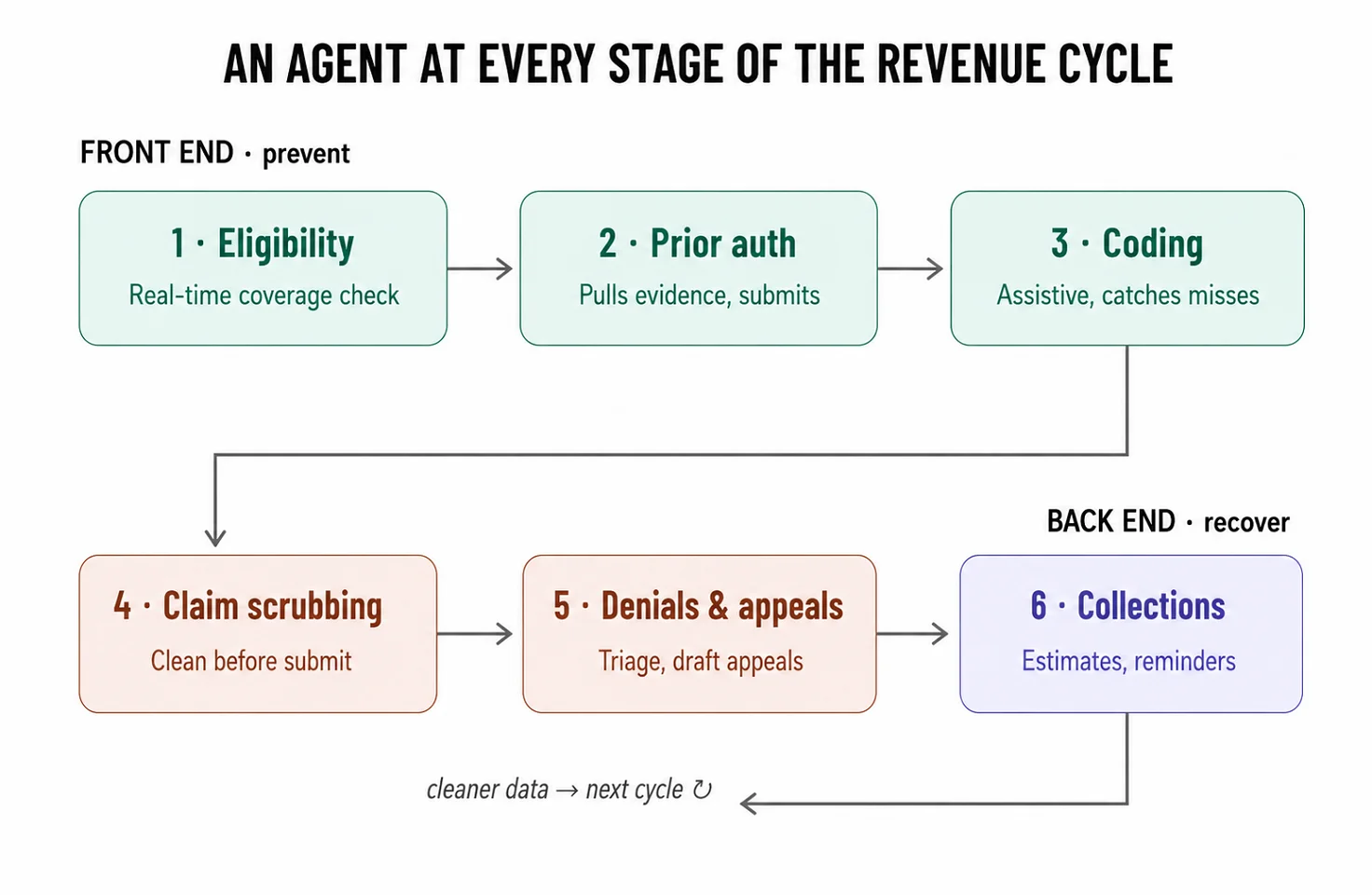
How It Works: An Agent at Every Stage of the Cycle
The revenue cycle isn't one task — it's a relay race, and revenue gets passed in the handoffs between runners. The value of an orchestrated agent is that it can run several legs of that race itself. Here's what that looks like at each stage, in the order money actually moves through a practice.
Eligibility and benefits verification
Everything downstream depends on getting this right, and it happens before the patient is even seen. The agent checks coverage in real time against the payer — active plan, covered services, copay, deductible, whether a referral or prior auth is required — and flags problems while there's still time to fix them. A patient whose coverage lapsed last month gets caught at scheduling, not three weeks later when the claim is rejected. Since registration and eligibility errors are the largest single source of denials, this is the cheapest stage at which to prevent revenue loss, and the one with the highest return on automation.
Prior authorization
Prior auth is the most painful administrative task in medicine, and the numbers confirm this. Physicians and their staff spend an average of 13 hours each week completing prior authorization requests, 40% of practices have staff who work exclusively on them, and 94% of physicians say it contributes to burnout.
An agent addresses this directly: it reads the chart to pull the clinical evidence a payer will want, pre-fills the payer's form with that evidence and citations back to the documentation. It then submits through whatever channel the payer uses, and tracks the request to a decision instead of letting it sit in someone's queue.
The regulatory wind is at your back here. The CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F) requires affected payers to return decisions within 72 hours for urgent requests and seven calendar days for standard ones — with those timeframes and denial-reason transparency starting in 2026, and FHIR-based prior authorization APIs required by January 1, 2027. As payers move from fax and phone to standardized APIs, an agent built to speak those APIs goes from a workaround to the native way the process runs.
One caveat worth knowing: the rule covers government plans — Medicare Advantage, Medicaid, CHIP, and QHP issuers — not commercial payers, so the fax machine isn't gone yet.
Medical coding and charge capture
Coding is where revenue quietly evaporates in two directions at once. Under-coding leaves money uncaptured for work that was actually done; over-coding invites denials and audit exposure. An agent works as an assistive coder, reading clinical documentation, suggesting the ICD-10 and CPT codes it supports, and flagging services that were documented but never charged. Just as useful is what it catches going the other way: codes that won't survive the payer's edits, caught before the claim goes out rather than after it comes back. The human coder stays in the loop and signs off; the agent removes the grind of combing through dense notes line by line.
Claim scrubbing and submission
Before a claim leaves the building, it should be checked against the specific payer's rules, and those rules are too numerous and change too often for anyone to remember. The agent validates each claim against current payer edits, fixes or flags what would trigger a rejection, and submits clean. The goal is a higher first-pass acceptance rate, which is the single metric that most directly shrinks the downstream denial pile. Every claim that goes out clean is one that never has to be reworked, and one that's reimbursed faster, because first-pass claims don't sit in a denial queue waiting on an appeal.
Denial management and appeals
When a denial does land, the agent triages it: classifying by root cause, grouping similar denials, and prioritizing by recoverable dollars so staff spend their effort where it pays off. For appealable denials, it assembles the appeal package — pulling the documentation, matching it to the denial reason, drafting the letter.
This matters because the appeal economics are wildly lopsided in the provider's favor, and almost nobody acts on it. In Medicare Advantage, more than 80% of appealed prior authorization denials were partially or fully overturned in 2024 — yet only about 11.5% of denied requests were ever appealed. Most denied revenue that could be won back is simply left on the table, because appealing by hand costs more than it's worth. An agent changes that math by making the appeal nearly free to produce.
Patient billing and collections
The last stretch of the cycle is increasingly where the money is, as more of the bill shifts onto patients. The agent gives patients clear, upfront cost estimates instead of a cryptic statement weeks later. It sends reminders through the channels people actually respond to and automatically offers payment plans for larger balances. Friendlier, clearer, and better-timed communication collects more than a stack of mailed statements — and it does it without adding to the front desk's workload.
Under the hood
These agents aren't one large model doing everything. A typical architecture splits the work. Lightweight, specialized parsers handle structured formats like X12 EDI, while a retrieval-augmented (RAG) layer over the clinical record (notes, problem lists, prior results) allows the agent to find and cite the evidence a prior authorization or appeal actually needs. The reasoning model orchestrates these tools and decides when to act and when to escalate, rather than generating answers from memory. That separation is also a safety property: the agent quotes the record instead of paraphrasing it, which is what makes its output auditable. And, as the next sections show, auditability is the whole game in a field where opaque automation is becoming a legal risk.
Integrating RCM Agents with Your Systems
Integration depth is what determines whether an RCM agent does the work or just talks about it. An agent that can read your systems but not write back to them is a very expensive dashboard. To actually move money, it has to do two things — read and write to your EHR and practice management system, and exchange transactions with payers. Most of the real engineering lives in that second half.
Connecting the agent
On the provider side, the agent reads and writes to the EHR and PMS — Epic, Oracle Health, athenahealth, and the rest — to pull clinical documentation, post charges, and update claim status. What it can reliably pull from the chart is defined by USCDI (US Core Data for Interoperability), the standardized set of clinical data classes — problems, procedures, notes, medications — that certified EHRs must expose. That standard is what makes evidence-gathering for prior auth predictable across systems, instead of a bespoke project per vendor.
The payer side is what makes RCM distinct. Decades of claims infrastructure run on X12 EDI transactions, and an RCM agent has to speak them fluently: the 270/271 pair for eligibility inquiry and response, the 837 for claim submission, the 835 for remittance advice (how payments and adjustments come back), and the 278 for prior authorization request and response. These aren't legacy curiosities you can route around. They are how the money actually moves today, and any agent that touches the back office has to handle them natively.
FHIR is the future; X12 is the present
Two standards coexist, and a serious integration prepares for both. X12 EDI is the present: it carries the overwhelming majority of claims and eligibility traffic right now, and it isn't going anywhere soon. FHIR (and specifically the prior authorization API mandated by CMS-0057-F) is the direction of travel, with government payers required to stand up FHIR-based PA APIs by 2027.
The practical implication is to build for X12 today and design for FHIR tomorrow. For the next several years, a single practice will run eligibility over X12 with one payer and FHIR with another, sometimes on the same day. But treat the standard as an adapter you build and maintain, not a hard-coded assumption — and don't underestimate that adapter. Translating between FHIR's clinical resources, like Claim and ExplanationOfBenefit, and X12's rigid EDI segments is real engineering: data mapping that must be correct every single time money moves. This is exactly why integration depth, not model quality, is where most RCM projects succeed or fail.
Patient matching and PHI boundaries
Before the agent posts anything, it has to be certain it's acting on the right patient's record. Match on multiple identifiers, never on name alone, and stop for human confirmation when confidence is low: a misattributed charge or a claim filed under the wrong record is a bigger problem than a duplicate appointment. PHI boundaries apply throughout — every system in the chain operates under a BAA, PHI is minimized in logs, and access is scoped to what each task actually requires.
Fitting into the billing team's workflow
Integration isn't only technical, it's organizational. In RCM, the human-in-the-loop isn't a nicety, it's the design. The cost of an error is high: a wrong code or a bad claim has compliance and audit consequences, so the right division of labor keeps people at the decision points that carry risk.
The agent takes the high-volume, rules-driven work — eligibility checks, claim scrubbing, status tracking, first-draft appeals — and escalates the judgment calls. This includes anything affecting coding integrity, edge-case denials, and any action above a dollar or risk threshold the practice sets. The agent prepares the work, and a person approves it: coders sign off on codes and billers approve appeals before they go out. But where they do that approving matters as much as the fact that they do it. The approval step has to live where the work already happens — inside the EHR or the billing queue, not in a separate tool — or the friction of switching screens quietly kills adoption. Building that write-back and approval flow into a closed system like Epic, through SMART on FHIR or a proprietary API, is among the harder parts of the project, and it's a large part of why the cautious, assist-mode rollout below exists.
Roll it out the way the risk demands: start in a shadow or assist mode where the agent drafts and a human approves everything, prove accuracy on a single workflow — eligibility is the usual first pick, high-volume and low-risk — then widen autonomy and scope as the numbers earn it.
Ready-Made Platforms vs. Custom Development
The RCM tooling market is far more crowded than most, and that changes the build-vs-buy question. Almost every major vendor now sells "agentic AI" for the revenue cycle — at HIMSS 2026, companies like Waystar, FinThrive, Innovaccer, Solventum, and most of the field announced agents that work prior auth, denials, and coding (HIMSS 2026 RCM recap). The EHRs themselves are turning into agent platforms: athenahealth ships 80+ AI RCM features inside athenaOne, and Epic previewed a no-code "Agent Factory." So the real question usually isn't whether a tool exists for your problem. It's whether the assembled tools fit how your organization actually bills.
What the platforms cover well
For a single stage of the cycle, ready-made is hard to beat. There are mature, specialized tools for almost every box on the map: Cohere Health for payer-policy-aware prior auth, Experian's Patient Access Curator for eligibility and front-end data, clearinghouse-grade scrubbing from Waystar and the like, and EHR-native modules that need no integration at all because they already live in your system of record. If your payer mix is standard and you want to fix one well-defined leak quickly, a platform gets you there in weeks.
Where custom earns its place
Custom development pays off when the value is in orchestration rather than any single step — stitching eligibility, auth, coding, and denials into one flow that hands off automatically instead of dumping each result back on staff. It also wins when your environment doesn't match the platform's assumptions: a non-standard or legacy EMR, specialty billing rules the templates don't handle, a multi-entity group with several systems, or data-control requirements that rule out sending PHI to a vendor's cloud.
One caution on the economics, because it cuts against a common assumption. Custom isn't free of variable cost. An agent that calls commercial LLM APIs still pays per token, and the clinical-document-heavy tasks — reading a full chart to support a prior auth, for instance — generate large context windows that aren't cheap, so your run cost still scales with claim volume. The difference is control: when you own the architecture, you can drive that cost down in ways a vendor's per-claim price won't allow — smaller specialized models for routine parsing, caching, retrieval that sends only the relevant excerpt instead of the whole record, or self-hosting. Per-transaction or per-seat platform pricing that's cheap in a pilot can still exceed a well-optimized custom build at volume, but "we own the code" and "we have no marginal cost" are not the same statement.
|
Ready-made platform |
Custom development |
|
|
Time to value |
Weeks for a single stage; pre-built payer and EHR connectors |
Months — discovery, integration, and pilot before payback |
|
Cost model |
Subscription or per-transaction; scales up with volume |
Upfront build plus maintenance; lower marginal cost per claim, but LLM/compute usage still scales with volume |
|
Integration depth |
Strong for major EHRs and standard payers; weaker on legacy and edge cases |
Built around your actual systems, including legacy and multi-entity setups |
|
Best at |
Quickly automating one well-defined stage |
Orchestrating multiple stages end to end |
|
Data control |
PHI processed in the vendor's environment under a BAA |
PHI stays in your infrastructure |
|
Customization |
Configurable within templates; complex rules may not fit |
Any rule you can document |
|
Vendor lock-in |
High — flows, data, and integrations live with the vendor |
Low — you own the code and can change hosting or partners |
The most common sensible path is hybrid: start with a platform on one high-volume stage to validate ROI fast, then build custom where orchestration across stages (or an awkward in-house system) is where the money is stuck. Buying and building aren't opposites here; the question is which stage deserves which.
Compliance, Safety, and Trust
RCM agents touch PHI and move money, which puts them under more scrutiny than almost any other healthcare automation, and the regulatory ground is shifting under them right now. Getting this layer right isn't a formality. It's what keeps an efficiency tool from becoming a liability.
The basics, applied to money and PHI
Every vendor in the chain, including the model provider, operates under a BAA; PHI is minimized in logs and transcripts; and access is scoped to the task. With third-party LLMs that point deserves to be sharper than a BAA alone: the deployment should run under a zero-data-retention arrangement, where the provider neither stores the protected health information sent to it beyond the moment of processing nor uses it to train its models. A BAA makes a vendor accountable for PHI; zero retention is what keeps that PHI from quietly becoming training data for a model you don't control. Because these agents act on financial records, two more things matter: an audit trail for every action the agent takes, and human approval at the points where an error has compliance weight.
Coding is where the human sign-off isn't optional
The sharpest version of that risk is coding. An agent reading an ambiguous note can misread a comorbidity as the primary diagnosis, or suggest a higher-acuity code than the documentation truly supports. Done once, that's an error. Done at scale without review, it's the pattern regulators call upcoding, and it carries False Claims Act exposure, regardless of whether anyone intended to overbill. This is the clearest reason a human sign-off stays in the loop: it's the difference between an efficiency gain and a fraud allegation, and it's the core of what revenue integrity teams exist to protect. The agent's job is to assemble and justify; the accountable decision stays with a person.
Payer-side AI is already drawing fire
This is the part most vendor content skips. Automated denial systems on the payer side are under active legal and regulatory pressure — class-action suits over algorithmic denials have made headlines, and CMS has moved to require that medical-necessity denials be reviewed by qualified clinicians. The lesson for a provider-side agent is to be the opposite of a black box: every flag and every appeal it generates should be explainable and traceable to a payer rule or a piece of documentation. An agent that can show its work is an asset in exactly the environment where opaque automation is becoming a legal risk.
Regulation as tailwind, not just constraint
CMS-0057-F is usually filed under "compliance burden," but for a well-built agent it's the opposite. By forcing payers onto standardized FHIR APIs and into hard decision deadlines, it replaces the fax-and-phone guesswork an agent has to fight today with structured, queryable interfaces it can use natively. The mandate that's a scramble for payers is, for a provider-side agent, the infrastructure it was waiting for.
The honest caveat on autonomy
There's a documented failure mode worth designing against. When providers and payers both deploy aggressive automation, prior auth can devolve into what PHTI calls "bot wars" — automated systems firing high-volume back-and-forth at each other without resolving the underlying clinical question (PHTI, Administrative AI, April 2026). The takeaway isn't to avoid automation. It's to aim at resolving a request correctly the first time rather than just submitting faster, which is a design choice you make up front.
Metrics and ROI
If you can't measure it against a baseline, you can't prove it worked — and in RCM, the baseline numbers are ones finance already tracks, which makes this easier than in most automation projects.
What to measure
The metrics that matter map directly onto the stages of the cycle: clean claim rate (or first-pass acceptance), initial denial rate, denial overturn rate, days in accounts receivable, net collection rate, cost to collect, prior authorization turnaround time, and staff hours spent on each. Capture them before go-live. The single most useful one is first-pass acceptance, because it sits upstream of almost everything else — every point of improvement there minimizes the denial pile downstream.
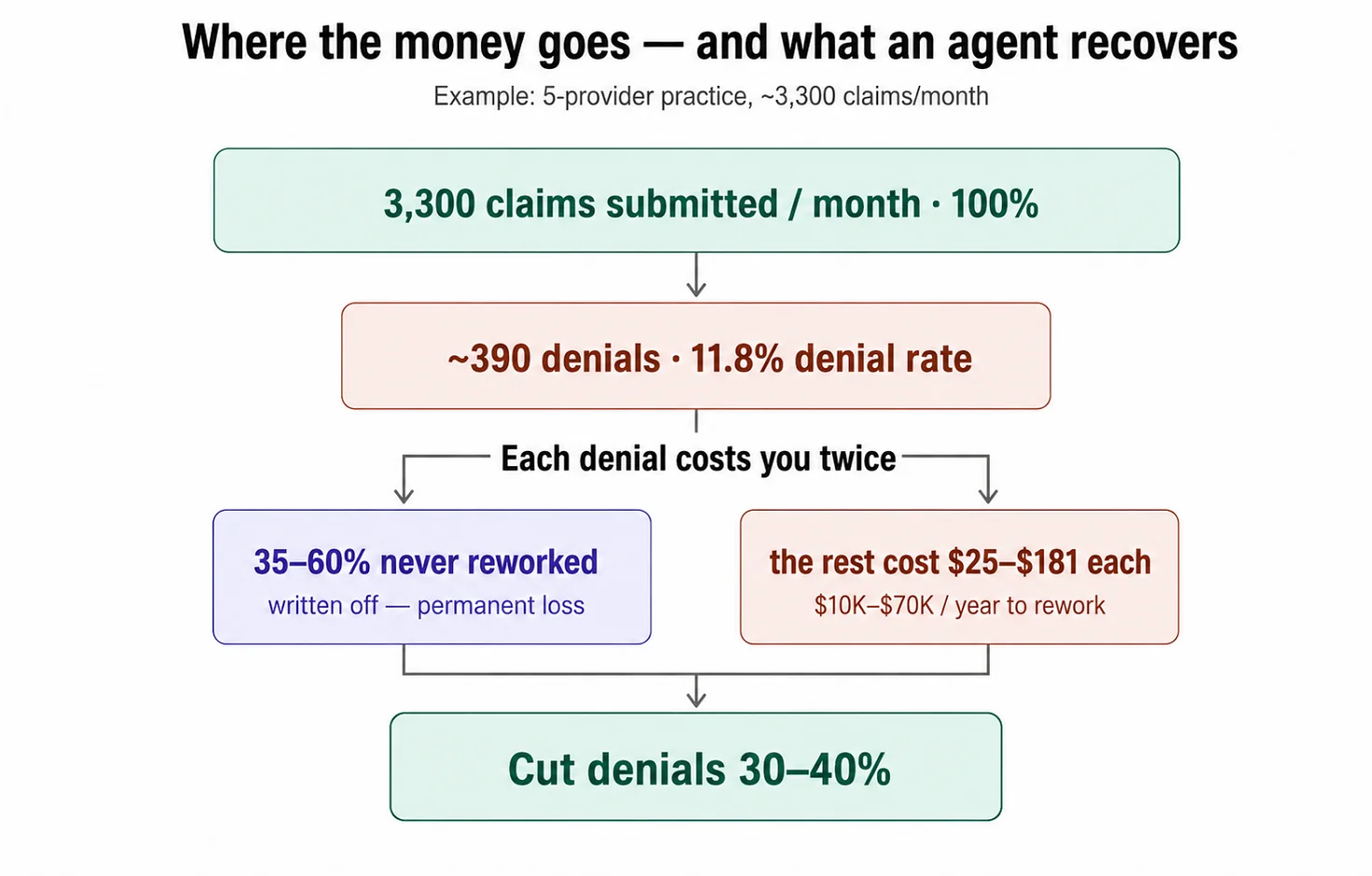
A worked example
Take a five-provider practice submitting roughly 3,300 claims a month at an 11.8% initial denial rate — about 390 denials a month, or some 4,700 a year. At a rework cost of $25 to $181 per claim, just processing those denials runs well into six figures annually — on the order of $120,000 even at the low practice rate, and far more where hospital-level costs apply — before counting the 35-60% that never get reworked and are written off entirely. Cut denials by 30-40% with cleaner front-end data and scrubbing, and you're removing 120-155 denials a month — the rework savings alone are real money, and the recovered write-offs are larger still. A frequently cited vendor case study (Experian's work with OhioHealth) reported a 42% drop in registration- and eligibility-related denials in the first year. Treat that as directional — it's vendor-reported and specific to front-end denials, not the whole cycle.
The AI cost paradox
Here's the finding that separates an honest ROI case from a sales pitch. A 2026 Peterson Health Technology Institute analysis found that AI can cut how much an individual organization pays to execute prior authorizations and billing — but there's no evidence yet that it lowers the average cost per claim once you factor in the price of the AI itself and the higher transaction volumes it generates. Faster is not the same as cheaper. The implication for your ROI model is concrete: measure the net effect — savings minus the fully loaded cost of the solution and any volume it adds — not just the speed-up on a single task. An agent that doubles your prior auth throughput while doubling your prior auth spend hasn't earned its keep, and the only way to know is to model net, not gross.
Set honest expectations
A 30-40% reduction in denials is a realistic planning range for the front-end and scrubbing work where the evidence is strongest. Bigger single-number results exist in vendor materials, but they're usually scoped to one denial category or one favorable starting point. Build your business case on the conservative figure and on the metrics finance already trusts, and let the upside be upside.
Implementation Roadmap
The pattern that works is the same one from scheduling, adapted for higher stakes: prove it on one stage, measure hard, then widen. Five steps.
- Discovery — and it's mostly accounting, not engineering. Pull your real baseline before anything else: initial denial rate, days in A/R, cost to collect, denial overturn rate. Then inventory your payer mix and the systems each stage touches. Without those numbers you'll have no way to prove the agent did anything — which is the most common reason these projects quietly fail to win renewal.
- Pick one stage to pilot. Resist the urge to automate the whole cycle at once. Eligibility is the usual first choice: high-volume, low-risk, and upstream of the most denials, so a win there shows up everywhere downstream. Denial management is the other strong candidate when a back-end backlog is the visible pain. One stage, one clear before-and-after.
- Integrate and run in assist mode. Connect the agent to the systems that each stage needs, then keep a human in the loop from day one — the agent drafts, a person approves. This is both a safety measure and one that builds trust: the billing team sees the agent's work before it goes live, and accuracy gets validated on real cases instead of in a demo.
- Measure against the baseline. Run the pilot for a defined window — long enough to clear normal billing cycles — and compare the same metrics you captured in Step 1. Net effect, not gross: include the fully loaded cost of the solution, not just the time saved (see the AI cost paradox above).
- Widen once the numbers hold. Only after the pilot proves out do you add adjacent stages, so the handoffs between them start to automate — which is where orchestration actually pays off. Expand autonomy and scope as the metrics earn it, not before.
A note on what goes wrong, because the failure modes are predictable: launching without a baseline (nothing to prove ROI against), automating everything at once instead of proving one stage, and pulling the human out of steps that carry compliance or dollar risk. None of these are technology problems. They're discipline problems — and the roadmap above exists to avoid all three.
Conclusion
The revenue cycle leaks at both ends — payer denials on the front, uncollected balances on the back — and most of those losses are administrative, not clinical. That's precisely why agents fit: the work is high-volume, rule-driven, and repetitive, and the regulatory shift toward standardized APIs is removing the friction that used to make automation rigid. The formula is simple to state and hard to execute: prevent denials at the front end, recover what's recoverable at the back, and collect what's owed — with a human at every step that carries real risk.
The two things that separate a working deployment from an expensive disappointment are the same two we've come back to throughout: integrate deeply enough that the agent can actually act, and measure net effect honestly enough to know whether it's working. Do both, and the gains show up in numbers your CFO already watches.
An RCM agent is also one piece of a larger picture. It sits alongside the scheduling and intake agents earlier in the patient journey, and each of its own stages — prior authorization, denial management — is deep enough to deserve its own treatment. If you're mapping where automation earns the most in your organization, the revenue cycle is usually where the clearest dollars are.
Frequently Asked Questions
How do AI agents reduce claim denials?
AI agents reduce denials by attacking them where they start — the front end. Most denials trace back to eligibility and registration errors made before a claim is ever submitted.The agent verifies coverage in real time, catches missing prior authorizations, and scrubs each claim against the specific payer's rules before it goes out. The result is a higher first-pass acceptance rate, which shrinks the denial pile downstream. When a denial does occur, the agent triages it by root cause and drafts the appeal, so recoverable revenue doesn't get written off. Realistic results land in the 30-40% denial-reduction range for the front-end and scrubbing work where the evidence is strongest.
Which RCM tasks can actually be automated?
A useful rule of thumb: automate the work that's high-volume and rules-driven; keep humans on the work that's judgment-driven. In practice that means the agent can carry most of the repetitive load across the cycle, while a human remains accountable for anything where an error has clinical or compliance consequences — final coding sign-off, contested denials, and approving outbound appeals. The test isn't "is this task technically automatable" (most are) but "what does it cost if the agent gets it wrong." Tasks where a mistake is cheap and reversible are the first to automate; tasks where a mistake creates audit exposure or a misfiled claim stay under human approval, with the agent preparing the work rather than finalizing it.
Does an RCM agent integrate with Epic, athenahealth, or other systems?
Yes. On the provider side, agents read from — and write to — major EHR and practice management systems, such as Epic, Oracle Health, athenahealth, eClinicalWorks, and others. On the payer side, they exchange the standard X12 EDI transactions that run the back office today (270/271 for eligibility, 837 for claims, 835 for remittance, 278 for prior authorization). The industry is also moving toward FHIR-based APIs — the CMS-0057-F rule requires government payers to support a FHIR prior authorization API by 2027 — so a well-built agent handles X12 now and is designed for FHIR as it arrives. Legacy systems without modern APIs can still be integrated through middleware or custom connectors, with extra discovery work.
Is AI-driven prior authorization compliant with CMS rules?
It can be, and the regulations are moving in its favor. CMS-0057-F requires affected payers to return prior authorization decisions within 72 hours for urgent requests and seven calendar days for standard ones, to give specific denial reasons, and to stand up standardized FHIR APIs by 2027 — all of which make automated, standards-based prior auth easier rather than harder. The compliance requirements that matter on the provider side are the usual ones: a BAA with every vendor in the chain, PHI minimized in logs, an audit trail for every action, and human review at decisions that carry clinical or compliance weight. The rule currently covers government plans — Medicare Advantage, Medicaid, CHIP, and QHP issuers — not commercial payers.
Will an RCM agent replace our billing staff?
No — it changes how they work. The agent absorbs the high-volume, repetitive load: eligibility checks, claim scrubbing, status tracking, first-draft appeals. Billers and coders move to the work that needs judgment — complex denials, coding integrity, payer escalations, and approving the agent's output before it goes out. In RCM specifically, keeping a human in the loop isn't optional, because the cost of an error is higher than a wasted appointment slot. Most organizations use the agent to handle volume their team can't keep up with, not to shrink the team.
How much does an RCM agent cost?
It depends on the model. Platform tools are typically priced per provider per month (roughly $200-$1,000+) or per claim ($3-$10), while full-service RCM outsourcing usually runs 6-10% of collections. Custom development, plus maintenance, is a larger upfront investment, but it eliminates per-transaction fees and pays off at higher claim volumes. The more useful number to anchor on is cost-to-collect: well-run organizations spend about 2-3% of revenue collecting it, against an industry average closer to 4-6%, so the right question isn't the sticker price, but whether a solution lowers your total cost-to-collect — measured net of its own cost.
What's a realistic denial-reduction target?
Start from your own baseline rather than a headline number. Pull your current initial denial rate and your top denial reasons before you do anything — a practice losing most of its denials to eligibility errors has a very different upside than one with a clean front end but slow appeals. As a planning range, 30-40% is defensible for front-end and scrubbing improvements, but the honest way to set your target is to size it against where your specific denials are coming from. Then measure the actual change against the baseline you captured. Be skeptical of any single percentage quoted without a starting point and a denial category attached to it.
Published on Jul 9, 2026





