EHR Replacement: Strategies for Cost Management and Data Preservation
Table of contents
- What This Transition Looks Like (The Shift in Reality)
The biggest fear when replacing an old clinical system is the chaotic "interim period." Leaders worry that during the months of migration, data will get lost, sync errors will corrupt billing codes, or the entire database will lock up, leaving doctors unable to access patient charts.
To eliminate this risk, modern migrations drop point-to-point connections entirely. Instead, we implement a Progressive Coexistence Stack. This decoupled architecture allows your old system and the new platform to operate simultaneously without interfering with one another.
Here is how this architecture functions under the hood to keep your day-to-day operations safe: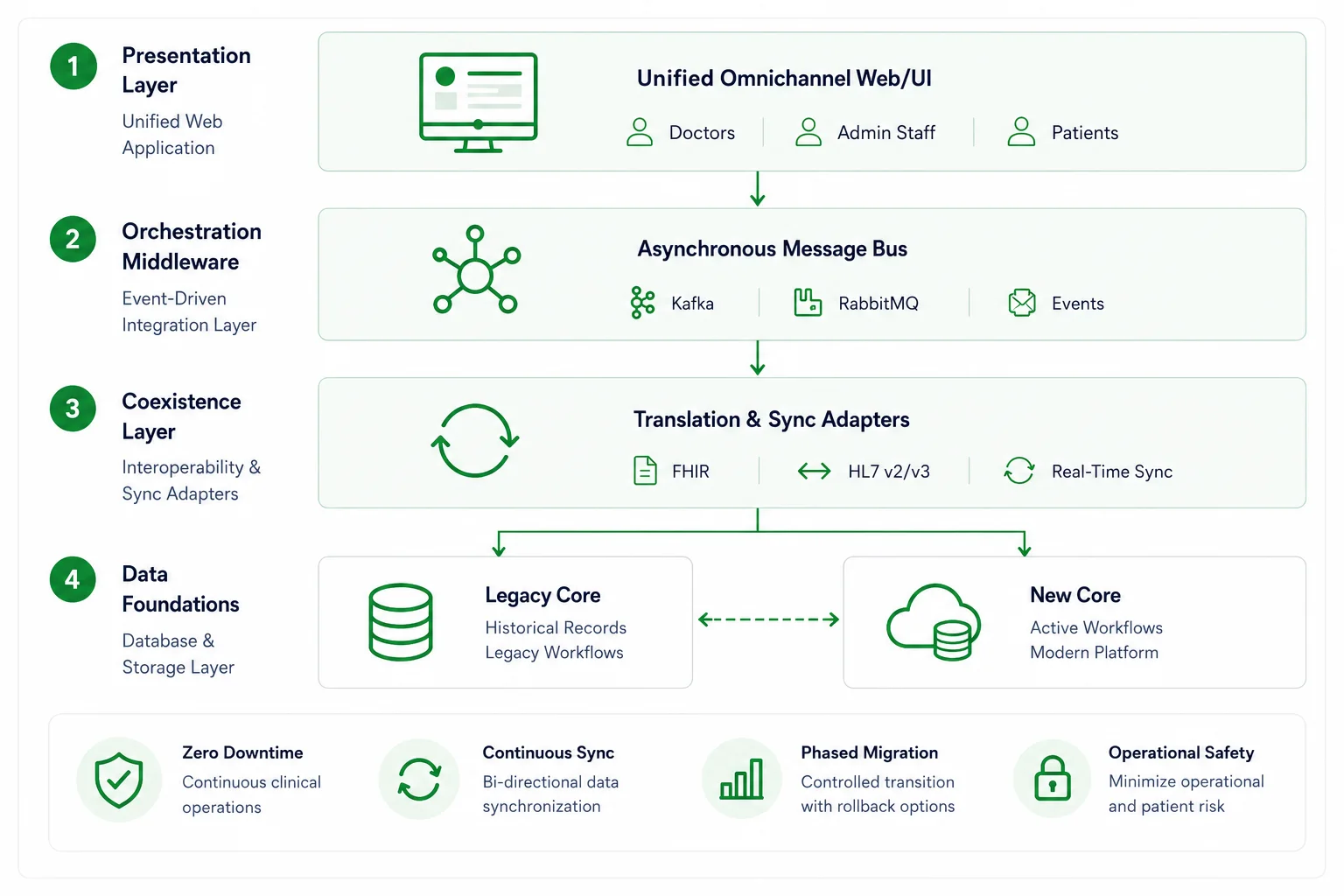
PROGRESSIVE COEXISTENCE STACK Presentation Layer Unified Omnichannel Web/UI Orchestration Middleware Asynchronous Message Bus Coexistence Layer Translation & Sync Adapters Data Foundations Legacy Core - New Core
1. Presentation Layer (Unified Web Application Interface)Your medical staff shouldn't have to log into two different systems or double-enter data during the transition. The presentation layer provides doctors and administrative staff with a single, clean browser-based interface. It doesn't care where the underlying data lives; it dynamically pulls patient info from whichever database holds the record, keeping the charting experience fluid and consistent.
2. Communication Middleware (Asynchronous Message Bus)
This layer acts as the absolute buffer for your system performance. Instead of sending raw requests directly to heavy transactional databases, all user actions (like booking a slot or editing a chart) are published as independent events to a message bus like Apache Kafka or RabbitMQ. If your legacy database experiences a temporary lag or slowdown during a data extraction batch, the middleware queue safely buffers the data payloads, preventing the user interface from freezing for your staff.
3. Interoperability Translators (Fast Healthcare Interoperability Resources & HL7 Adapters)
Legacy platforms and modern cloud databases speak completely different languages. This translation tier utilizes real-time sync adapters to automatically convert fragmented, proprietary legacy data formats into standard, globally compliant data structures on the fly. This ensures that records modified on either side are immediately understandable by both systems.
4. Storage Foundations (The Coexistence Engine)
At the bottom of the stack sit your actual data engines: the legacy system and the next-generation core platform. Instead of attempting a single-day full core replacement, this foundation supports phased data routing. Active patient profiles and high-concurrency workflows are incrementally shifted to the new core section by section, while older historical records remain insulated until they are ready for archiving.
Why Most Legacy Replacement Projects Get StuckThe biggest misconception about modernizing healthcare software is that the technology itself is the hardest part. In reality, most projects fail or stall because of everyday operational realities, not coding limitations.
Your clinical teams have years of muscle memory built around the old platform. Your billing department knows exactly how to navigate its quirks to get claims paid. If a modernization project focuses purely on flashy features and ignores how your staff actually works, you will face immediate resistance, productivity drops, and a surge in internal support tickets.
The most common traps include:
- Treating data cleanup as an afterthought (leading to broken records later).
- Attempting a single-day "big bang" switch that paralyzes clinic workflows.
- Forgetting that doctors need to see a patient’s historical timeline instantly.
- Getting hit with massive, unexpected fees from your old vendor just to extract your data.
To make your upgrade succeed, you have to treat it as a multi-phase operational transition rather than an overnight software replacement.
The True, Hidden Drain of an Aging System
Maintaining an old EHR platform often looks like the safer, cheaper choice on paper. But if you look closer at your weekly operations, you’ll find that the old core is quietly bleeding cash in four distinct areas:
1. The Skyrocketing Maintenance Trap
Legacy software depends on outdated technologies and proprietary codebases. As engineers who understand these older systems retire or move on, finding someone to fix a bug becomes incredibly difficult. Old vendors know this, and they continuously raise their support fees simply to keep your existing, basic functionality operational.
2. The Interoperability Brick Wall
Modern healthcare relies on immediate, real-time data exchange. If your clinical core cannot communicate natively via modern Fast Healthcare Interoperability Resources application program interfaces, sharing data with outside laboratories, pharmacy networks, or imaging centers becomes a nightmare. Your staff ends up wasting hours on manual file exports, faxes, and fragile custom workarounds that break constantly.
3. The Vendor Data Lock-In Surprise
One of the most frustrating moments in a modernization project is discovering you don't fully control your data. Many legacy vendors purposefully store patient records in proprietary formats that make extraction slow and expensive. Gaining access to your own decades of historical records can quickly become one of the largest, most unexpected line items in your migration budget.
4. Revenue Cycle Inefficiencies
An outdated system slows down everything, including your payments. If your platform cannot automate insurance eligibility checks or apply live validation to diagnostic coding models, your billing team has to process claims manually. This drives up coding mistakes, delays submissions, and directly increases insurance claim denials.
Legacy EHR Replacement Costs: Budgeting for System Modernization
Replacing a legacy EHR system is rarely a simple software purchase. In most healthcare organizations, the largest expenses come from data migration, integration engineering, clinical workflow redesign, and operational risk mitigation rather than the new software platform itself.
A realistic modernization budget should account for five distinct phases: data preparation, system engineering, transition management, compliance readiness, and parallel operations. Understanding where the financial resources go helps leadership teams avoid one of the most common mistakes in healthcare modernization - underestimating the true cost of migration while overestimating the standalone cost of the software.
Here is exactly where your financial resources will be allocated during a custom replacement program:
1. Data Auditing and Cleanup (15% to 20% of Total Budget)
Before any migration begins, organizations need a clear understanding of what data actually exists inside the legacy environment. Historical patient records often contain duplicate profiles, inconsistent clinical coding standards, incomplete demographic information, retired medical terminology, and broken historical references.
This phase includes comprehensive data inventory and mapping, record quality assessments, extraction planning, automated validation rules, and test migration exercises. Many healthcare organizations discover critical data quality issues during this stage that would otherwise surface during go-live and severely disrupt clinical operations.
2. Integration and Middleware Engineering (40% to 50% of Total Budget)
This is typically the largest investment category. Modern healthcare ecosystems depend on dozens of interconnected systems, including Laboratory Information Systems, Pharmacy Management Platforms, Medical Imaging Repositories, Revenue Cycle Management Systems, insurance eligibility validation services, patient web portals, and mobile applications.
Rather than creating fragile, direct point-to-point connections, modern architectures use integration middleware, event-driven microservices, and Fast Healthcare Interoperability Resources-based application programming interfaces. The objective is not simply to migrate data - it is to create an infrastructure that remains highly flexible for future integrations, facility expansions, and healthcare acquisitions.
3. Historical Data Archiving and Infrastructure Optimization (10% to 15% of Total Budget)
One of the most expensive mistakes organizations make is attempting to move decades of historical records directly into a new production environment. In practice, older historical data is rarely accessed but must remain fully available for legal, clinical, and regulatory auditing purposes.
A dedicated cold archive strategy includes setting up immutable storage repositories, establishing long-term retention policies, deploying fast search and retrieval interfaces, and implementing audit-ready role-based access controls. This approach reduces live database complexity, improves everyday application performance, and dramatically lowers long-term cloud infrastructure costs.
4. Training, Adoption, and Compliance Readiness (15% to 20% of Total Budget)
Healthcare technology projects succeed or fail based on staff adoption. Even a technically flawless EHR platform will struggle if clinicians, nurses, or billing teams are not comfortable navigating the new workflows.
Organizations must budget for role-based staff training, isolated sandbox environments, real-world workflow simulations, clinical super-user mentorship programs, security awareness training, independent compliance readiness audits, and rigorous penetration testing. Investments in user adoption often generate a far greater return than investments in additional software features.
5. The Hidden Cost Most Budgets Miss: Parallel Operations (5% to 10% of Total Budget)
During large-scale migrations, healthcare organizations often operate both the legacy software and the new platform simultaneously for several months. This coexistence period creates temporary dual-run costs that are frequently overlooked during early planning stages.
These unexpected drains include maintaining legacy vendor contracts, supporting duplicate integration flows, running parallel cloud infrastructure environments, managing additional help desk technical staffing, and executing constant data reconciliation activities. For large provider networks, dual-run operations can easily account for a significant portion of the overall project budget. However, this temporary expense is usually far less costly than the catastrophic operational risk associated with a single-day "big bang" cutover.
Typical Budget Allocation Breakdown
This financial matrix displays the standard resource distribution required to execute a secure, risk-mitigated system transition:
Cost Category Typical Share of Budget Data Auditing and Cleanup 15%–20% Integration and Middleware Engineering 40%–50% Historical Data Archiving and Optimization 10%–15% Training, Adoption, and Compliance Readiness 15%–20% Parallel Operations and Contingency Funds 5%–10% The most successful modernization programs do not focus on replacing software. They focus on reducing long-term operational risk. When budgeting for a legacy EHR replacement, healthcare organizations should evaluate not only initial implementation costs, but also data quality, interoperability requirements, clinician adoption, and long-term infrastructure sustainability. These factors ultimately determine whether the project delivers lasting value or becomes another costly technology refresh cycle.
Data Preservation: Managing Active Records vs. Cold Archives
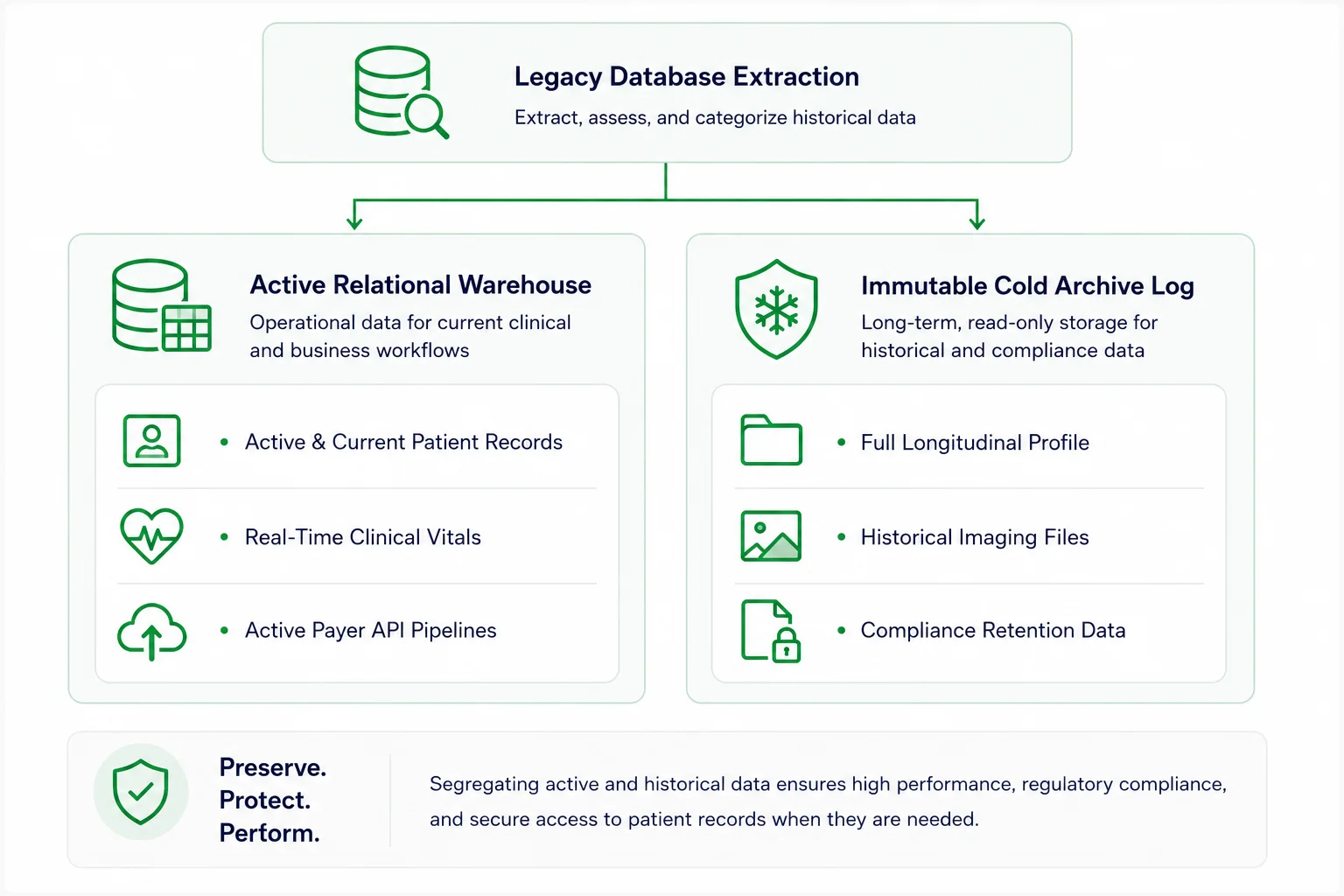
The single highest-risk moment in any system replacement project is data preservation. Your organization is legally and ethically responsible for decades of clinical documentation, lab results, imaging files, insurance claims, and immutable audit logs.
But here is a practical secret: attempting to force thirty years of unvalidated, messy historical logs into your brand-new transactional core is a major mistake. It complicates the migration and permanently slows down your new system's chart loading speeds. Instead, smart engineering teams split the data into two clear pipelines:
Active Clinical Data (The New Core)
This includes the essential information required for ongoing patient care. You parse, clean, and migrate only what is active: current patient profiles, active treatment plans, and recent clinical encounters from the last three years. This keeps your new database light, fast, and agile.
Historical Records (The Cold Archive)
What about the rest of the data? Medical compliance rules state you must keep records for years, but that doesn't mean they need to sit in your active system. Route older histories into a secure, low-cost immutable cold archive. This repository keeps the data completely read-only and audit-ready. If a doctor ever needs to see an old file, they can pull it up in a click, but it won't clutter or slow down your daily operations.
Emerline Case in Point (Custom Healthcare Engineering): Engineering a standalone medical ecosystem requires absolute synchronization across clinical, financial, and diagnostic modules. By delivering an enterprise-grade Custom EHR with robust, decoupled integration layers, custom charting views, and automated regulatory validation pipelines, our team completely resolved the usability and performance bottlenecks commonly found in off-the-shelf software packages, ensuring seamless data flow and clinical scalability for the provider.
De-Risking the Launch: The Coexistence Model
The fastest way to cause a operational crisis is to attempt a "big bang" migration - shutting off the old system on a Sunday night and expecting everyone to use the new one on Monday morning.
Instead, a progressive sidecar migration strategy lets you transition safely. The new cloud-native platform runs right alongside your legacy software. We deploy an asynchronous message bus (like Apache Kafka) as a bridge, allowing an api gateway to route traffic gradually.
For instance, you can onboard new patients or route a single department (like outpatient care) through the new core first, while keeping inpatient services on the old system. You move your books of business in incremental, controlled waves. If an integration quirk appears, your blast radius is tiny, and you have instant rollback options without disrupting the rest of the clinic.
To see how specialized user interfaces and transition frameworks keep clinical teams moving forward during a platform switch, visit our Emerline EMR and EHR Systems Framework page.
When pulling data out of a legacy database, never build direct point-to-point connections to your new core. It’s too risky.
Use an intermediate event streaming layer. Let the legacy platform dump its raw data into a secure queue, and use independent validation services to clean, format, and verify the records before they ever touch your new database. This keeps legacy formatting errors from corrupting your clean new environment.
Security, Privacy, and Keeping the Trust
Upgrading your clinical software means managing highly sensitive Protected Health Information. Security cannot be a final checklist item; it must be treated as a core design requirement from day one.
Encryption and Access Logs
Whether your data is sitting in your database or moving across networks, it must be completely locked down. Use Advanced Encryption Standard 256 keys at rest and TLS 1.3 encryption protocols in transit to ensure full Health Insurance Portability and Accountability Act and General Data Protection Regulation compliance. Your system must also generate automated, unalterable audit logs that track exactly who looked at, updated, or moved a patient's file.
Zero-Trust Access Isolation
To protect data privacy during the multi-phase changeover window, enforce strict Role-Based Access Control and Multi-Factor Authentication. This access framework ensures that physicians see clinical charts, billing teams access invoicing data, and data migration tools can only interact with their specific data buckets - keeping different user roles completely isolated inside the environment.
Emerline Case in Point (Ecosystem Compliance): Migrating complex data reporting streams away from legacy databases requires strict technical governance. Emerline handled this by building a highly secure, enterprise-scale Scalable Analytics Platform for Digital Healthcare. By constructing robust role-based access frameworks and secure data ingestion adapters, we removed legacy reporting bottlenecks while keeping sensitive clinical files private, encrypted, and audit-compliant.
Never let migrated patient charts or financial histories sit in browser cache or local device logs during your team testing windows.
Implement a data tokenization layer. When a provider opens a record, the interface should load a temporary tokenized string that destroys itself the moment they close the tab or log out. This zero-footprint web pattern protects your data assets even if a clinician’s physical laptop is lost or compromised.
Reality Check: What It Takes to Modernize
The true investment timeline and budget for a legacy replacement depend entirely on your data volume, the number of internal workflows, and the state of your existing databases.
Organizational Scale
Typical Transition Timeline
Typical Investment Budget
Small Outpatient Clinic
6 to 9 Months
$150,000 to $500,000
Multi-Site Specialty Practice
9 to 12 Months
$500,000 to $1,500,000
Regional Provider Network
12 to 18 Months
$1,000,000 to $5,000,000
Enterprise Hospital System
12 to 24 Months
$2,000,000+
Operational Readiness: Are You Ready to Migrate?
Your technical steering committee can use this working matrix to check if your infrastructure is prepared for data extraction and system modernization.
Target Area
Core Operational Requirement
Ready? (Yes/No)
Data Inventory
We have mapped every historical patient record and data silo across facilities.
Quality Audit
We ran an initial data quality assessment to identify corrupted or empty fields.
Interoperability
Our target database schemas are designed around native FHIR api web services.
Archive Policy
A strict, legally compliant data preservation retention policy has been approved.
Integration Map
Every required laboratory, pharmacy, and payer API integration is fully documented.
Access Control
Logins require Multi-Factor Authentication and strict role-based data isolation.
Session Security
Communication uses a Zero-Footprint pattern to disable local device data caching.
Failover Procedures
Step-by-step rollback paths are fully documented for every phase of rollout.
Connected Ecosystem Insights
Building a reliable, fast clinical platform requires matching great database engineering with scalable communication channels and smart user psychology.
- Integrating Virtual Care Natively: Adding real-time telehealth options directly into your custom platform requires a highly scalable, low-latency infrastructure design. Review our framework: Emerline Telehealth Development Roadmap.
- Minimizing Cloud Overhead Costs: Discover how custom interface engineering and self-service modules reduce long-term operating expenses: How a User-Friendly App Reduces Healthcare Costs.
Frequently Asked Questions
1. Should we migrate all historical patient data into our new system?
Practically speaking, no. Moving decades of messy, unvalidated data into your new platform slows down performance and complicates development. The cleanest strategy is to migrate active clinical data from the last three years into the new platform, while routing the rest into a secure, low-cost read-only cold archive for compliance audits.
2. How do we prevent duplicate data entry while running two systems at once?
We use real-time integration middleware. When a doctor or administrative staff member updates a patient chart or logs an appointment on one platform, the middleware instantly captures that event and replicates the data change across the parallel core, keeping both platforms synchronized automatically.
3. Can our clinicians access web-native health portals safely on mobile devices?
Yes, provided you implement the right security architecture. Mobile browser security relies on entirely disabling local data storage on the phone, utilizing biometric validation via WebAuthn protocols, and enforcing aggressive session expiration windows.
4. What are the actual risks of a failed or incomplete data preservation audit?
The consequences are severe. Violating health data retention laws can land you with millions of dollars in regulatory fines, immediate loss of your processing licenses from health authorities, complex legal lawsuits, and a permanent blow to market trust.
5. How does a modern system verify insurance eligibility automatically?
The backend uses automated Electronic Data Interchange transactions to ping insurance databases through secure web connections the moment a patient books a slot. Within seconds, the portal reads the response and updates the screen with exact copay details, completely eliminating manual verification calls.
Summary: Focus on Data Agility
Let’s be honest: healthcare leaders rarely wake up and decide to replace an Electronic Health Record (EHR) system just because they want a shiny new software interface.
Usually, the decision is forced by years of compounding frustration. You realize you are paying astronomical fees to an old vendor just to keep the system from crashing. Your doctors complain daily that the software requires too many clicks and distracts them from actual patient care. To make matters worse, every time you try to connect a modern tool - like a telehealth platform or a fast billing portal - the old database pushes back with errors.
If you are running an EHR system that was deployed 10 or 15 years ago, you are dealing with an operational bottleneck, not an asset. Over time, these systems accumulate a messy web of custom workarounds and unsupported patches. Eventually, a critical question arises: Is maintaining the old system truly cheaper than replacing it? For most growing healthcare organizations, the answer is already a clear no.
The real catch is that replacing a legacy EHR platform isn't just a simple software installation. It is a massive data migration, an operational shift, and a regulatory compliance challenge all happening at the same time. This guide breaks down how to navigate this transition safely, protect your historical records, and make sure your clinic keeps running smoothly from day one.
Before we jump into the strategy, take a look at how our teams design and launch modern medical environments on the Emerline Healthcare Industry Solutions page.
What This Transition Looks Like (The Shift in Reality)
The biggest fear when replacing an old clinical system is the chaotic "interim period." Leaders worry that during the months of migration, data will get lost, sync errors will corrupt billing codes, or the entire database will lock up, leaving doctors unable to access patient charts.
To eliminate this risk, modern migrations drop point-to-point connections entirely. Instead, we implement a Progressive Coexistence Stack. This decoupled architecture allows your old system and the new platform to operate simultaneously without interfering with one another.
Here is how this architecture functions under the hood to keep your day-to-day operations safe:
| PROGRESSIVE COEXISTENCE STACK | |
| Presentation Layer | Unified Omnichannel Web/UI |
| Orchestration Middleware | Asynchronous Message Bus |
| Coexistence Layer | Translation & Sync Adapters |
| Data Foundations | Legacy Core - New Core |
1. Presentation Layer (Unified Web Application Interface)
Your medical staff shouldn't have to log into two different systems or double-enter data during the transition. The presentation layer provides doctors and administrative staff with a single, clean browser-based interface. It doesn't care where the underlying data lives; it dynamically pulls patient info from whichever database holds the record, keeping the charting experience fluid and consistent.
2. Communication Middleware (Asynchronous Message Bus)
This layer acts as the absolute buffer for your system performance. Instead of sending raw requests directly to heavy transactional databases, all user actions (like booking a slot or editing a chart) are published as independent events to a message bus like Apache Kafka or RabbitMQ. If your legacy database experiences a temporary lag or slowdown during a data extraction batch, the middleware queue safely buffers the data payloads, preventing the user interface from freezing for your staff.
3. Interoperability Translators (Fast Healthcare Interoperability Resources & HL7 Adapters)
Legacy platforms and modern cloud databases speak completely different languages. This translation tier utilizes real-time sync adapters to automatically convert fragmented, proprietary legacy data formats into standard, globally compliant data structures on the fly. This ensures that records modified on either side are immediately understandable by both systems.
4. Storage Foundations (The Coexistence Engine)
At the bottom of the stack sit your actual data engines: the legacy system and the next-generation core platform. Instead of attempting a single-day full core replacement, this foundation supports phased data routing. Active patient profiles and high-concurrency workflows are incrementally shifted to the new core section by section, while older historical records remain insulated until they are ready for archiving.
Why Most Legacy Replacement Projects Get Stuck
The biggest misconception about modernizing healthcare software is that the technology itself is the hardest part. In reality, most projects fail or stall because of everyday operational realities, not coding limitations.
Your clinical teams have years of muscle memory built around the old platform. Your billing department knows exactly how to navigate its quirks to get claims paid. If a modernization project focuses purely on flashy features and ignores how your staff actually works, you will face immediate resistance, productivity drops, and a surge in internal support tickets.
The most common traps include:
- Treating data cleanup as an afterthought (leading to broken records later).
- Attempting a single-day "big bang" switch that paralyzes clinic workflows.
- Forgetting that doctors need to see a patient’s historical timeline instantly.
- Getting hit with massive, unexpected fees from your old vendor just to extract your data.
To make your upgrade succeed, you have to treat it as a multi-phase operational transition rather than an overnight software replacement.
The True, Hidden Drain of an Aging System
Maintaining an old EHR platform often looks like the safer, cheaper choice on paper. But if you look closer at your weekly operations, you’ll find that the old core is quietly bleeding cash in four distinct areas:
1. The Skyrocketing Maintenance Trap
Legacy software depends on outdated technologies and proprietary codebases. As engineers who understand these older systems retire or move on, finding someone to fix a bug becomes incredibly difficult. Old vendors know this, and they continuously raise their support fees simply to keep your existing, basic functionality operational.
2. The Interoperability Brick Wall
Modern healthcare relies on immediate, real-time data exchange. If your clinical core cannot communicate natively via modern Fast Healthcare Interoperability Resources application program interfaces, sharing data with outside laboratories, pharmacy networks, or imaging centers becomes a nightmare. Your staff ends up wasting hours on manual file exports, faxes, and fragile custom workarounds that break constantly.
3. The Vendor Data Lock-In Surprise
One of the most frustrating moments in a modernization project is discovering you don't fully control your data. Many legacy vendors purposefully store patient records in proprietary formats that make extraction slow and expensive. Gaining access to your own decades of historical records can quickly become one of the largest, most unexpected line items in your migration budget.
4. Revenue Cycle Inefficiencies
An outdated system slows down everything, including your payments. If your platform cannot automate insurance eligibility checks or apply live validation to diagnostic coding models, your billing team has to process claims manually. This drives up coding mistakes, delays submissions, and directly increases insurance claim denials.
Legacy EHR Replacement Costs: Budgeting for System Modernization
Replacing a legacy EHR system is rarely a simple software purchase. In most healthcare organizations, the largest expenses come from data migration, integration engineering, clinical workflow redesign, and operational risk mitigation rather than the new software platform itself.
A realistic modernization budget should account for five distinct phases: data preparation, system engineering, transition management, compliance readiness, and parallel operations. Understanding where the financial resources go helps leadership teams avoid one of the most common mistakes in healthcare modernization - underestimating the true cost of migration while overestimating the standalone cost of the software.
Here is exactly where your financial resources will be allocated during a custom replacement program:
1. Data Auditing and Cleanup (15% to 20% of Total Budget)
Before any migration begins, organizations need a clear understanding of what data actually exists inside the legacy environment. Historical patient records often contain duplicate profiles, inconsistent clinical coding standards, incomplete demographic information, retired medical terminology, and broken historical references.
This phase includes comprehensive data inventory and mapping, record quality assessments, extraction planning, automated validation rules, and test migration exercises. Many healthcare organizations discover critical data quality issues during this stage that would otherwise surface during go-live and severely disrupt clinical operations.
2. Integration and Middleware Engineering (40% to 50% of Total Budget)
This is typically the largest investment category. Modern healthcare ecosystems depend on dozens of interconnected systems, including Laboratory Information Systems, Pharmacy Management Platforms, Medical Imaging Repositories, Revenue Cycle Management Systems, insurance eligibility validation services, patient web portals, and mobile applications.
Rather than creating fragile, direct point-to-point connections, modern architectures use integration middleware, event-driven microservices, and Fast Healthcare Interoperability Resources-based application programming interfaces. The objective is not simply to migrate data - it is to create an infrastructure that remains highly flexible for future integrations, facility expansions, and healthcare acquisitions.
3. Historical Data Archiving and Infrastructure Optimization (10% to 15% of Total Budget)
One of the most expensive mistakes organizations make is attempting to move decades of historical records directly into a new production environment. In practice, older historical data is rarely accessed but must remain fully available for legal, clinical, and regulatory auditing purposes.
A dedicated cold archive strategy includes setting up immutable storage repositories, establishing long-term retention policies, deploying fast search and retrieval interfaces, and implementing audit-ready role-based access controls. This approach reduces live database complexity, improves everyday application performance, and dramatically lowers long-term cloud infrastructure costs.
4. Training, Adoption, and Compliance Readiness (15% to 20% of Total Budget)
Healthcare technology projects succeed or fail based on staff adoption. Even a technically flawless EHR platform will struggle if clinicians, nurses, or billing teams are not comfortable navigating the new workflows.
Organizations must budget for role-based staff training, isolated sandbox environments, real-world workflow simulations, clinical super-user mentorship programs, security awareness training, independent compliance readiness audits, and rigorous penetration testing. Investments in user adoption often generate a far greater return than investments in additional software features.
5. The Hidden Cost Most Budgets Miss: Parallel Operations (5% to 10% of Total Budget)
During large-scale migrations, healthcare organizations often operate both the legacy software and the new platform simultaneously for several months. This coexistence period creates temporary dual-run costs that are frequently overlooked during early planning stages.
These unexpected drains include maintaining legacy vendor contracts, supporting duplicate integration flows, running parallel cloud infrastructure environments, managing additional help desk technical staffing, and executing constant data reconciliation activities. For large provider networks, dual-run operations can easily account for a significant portion of the overall project budget. However, this temporary expense is usually far less costly than the catastrophic operational risk associated with a single-day "big bang" cutover.
Typical Budget Allocation Breakdown
This financial matrix displays the standard resource distribution required to execute a secure, risk-mitigated system transition:
| Cost Category | Typical Share of Budget |
| Data Auditing and Cleanup | 15%–20% |
| Integration and Middleware Engineering | 40%–50% |
| Historical Data Archiving and Optimization | 10%–15% |
| Training, Adoption, and Compliance Readiness | 15%–20% |
| Parallel Operations and Contingency Funds | 5%–10% |
The most successful modernization programs do not focus on replacing software. They focus on reducing long-term operational risk. When budgeting for a legacy EHR replacement, healthcare organizations should evaluate not only initial implementation costs, but also data quality, interoperability requirements, clinician adoption, and long-term infrastructure sustainability. These factors ultimately determine whether the project delivers lasting value or becomes another costly technology refresh cycle.
Data Preservation: Managing Active Records vs. Cold Archives
The single highest-risk moment in any system replacement project is data preservation. Your organization is legally and ethically responsible for decades of clinical documentation, lab results, imaging files, insurance claims, and immutable audit logs.
But here is a practical secret: attempting to force thirty years of unvalidated, messy historical logs into your brand-new transactional core is a major mistake. It complicates the migration and permanently slows down your new system's chart loading speeds. Instead, smart engineering teams split the data into two clear pipelines:
Active Clinical Data (The New Core)
This includes the essential information required for ongoing patient care. You parse, clean, and migrate only what is active: current patient profiles, active treatment plans, and recent clinical encounters from the last three years. This keeps your new database light, fast, and agile.
Historical Records (The Cold Archive)
What about the rest of the data? Medical compliance rules state you must keep records for years, but that doesn't mean they need to sit in your active system. Route older histories into a secure, low-cost immutable cold archive. This repository keeps the data completely read-only and audit-ready. If a doctor ever needs to see an old file, they can pull it up in a click, but it won't clutter or slow down your daily operations.
Emerline Case in Point (Custom Healthcare Engineering): Engineering a standalone medical ecosystem requires absolute synchronization across clinical, financial, and diagnostic modules. By delivering an enterprise-grade Custom EHR with robust, decoupled integration layers, custom charting views, and automated regulatory validation pipelines, our team completely resolved the usability and performance bottlenecks commonly found in off-the-shelf software packages, ensuring seamless data flow and clinical scalability for the provider.
De-Risking the Launch: The Coexistence Model
The fastest way to cause a operational crisis is to attempt a "big bang" migration - shutting off the old system on a Sunday night and expecting everyone to use the new one on Monday morning.
Instead, a progressive sidecar migration strategy lets you transition safely. The new cloud-native platform runs right alongside your legacy software. We deploy an asynchronous message bus (like Apache Kafka) as a bridge, allowing an api gateway to route traffic gradually.
For instance, you can onboard new patients or route a single department (like outpatient care) through the new core first, while keeping inpatient services on the old system. You move your books of business in incremental, controlled waves. If an integration quirk appears, your blast radius is tiny, and you have instant rollback options without disrupting the rest of the clinic.
To see how specialized user interfaces and transition frameworks keep clinical teams moving forward during a platform switch, visit our Emerline EMR and EHR Systems Framework page.
When pulling data out of a legacy database, never build direct point-to-point connections to your new core. It’s too risky.
Use an intermediate event streaming layer. Let the legacy platform dump its raw data into a secure queue, and use independent validation services to clean, format, and verify the records before they ever touch your new database. This keeps legacy formatting errors from corrupting your clean new environment.
Security, Privacy, and Keeping the Trust
Upgrading your clinical software means managing highly sensitive Protected Health Information. Security cannot be a final checklist item; it must be treated as a core design requirement from day one.
Encryption and Access Logs
Whether your data is sitting in your database or moving across networks, it must be completely locked down. Use Advanced Encryption Standard 256 keys at rest and TLS 1.3 encryption protocols in transit to ensure full Health Insurance Portability and Accountability Act and General Data Protection Regulation compliance. Your system must also generate automated, unalterable audit logs that track exactly who looked at, updated, or moved a patient's file.
Zero-Trust Access Isolation
To protect data privacy during the multi-phase changeover window, enforce strict Role-Based Access Control and Multi-Factor Authentication. This access framework ensures that physicians see clinical charts, billing teams access invoicing data, and data migration tools can only interact with their specific data buckets - keeping different user roles completely isolated inside the environment.
Emerline Case in Point (Ecosystem Compliance): Migrating complex data reporting streams away from legacy databases requires strict technical governance. Emerline handled this by building a highly secure, enterprise-scale Scalable Analytics Platform for Digital Healthcare. By constructing robust role-based access frameworks and secure data ingestion adapters, we removed legacy reporting bottlenecks while keeping sensitive clinical files private, encrypted, and audit-compliant.
Never let migrated patient charts or financial histories sit in browser cache or local device logs during your team testing windows.
Implement a data tokenization layer. When a provider opens a record, the interface should load a temporary tokenized string that destroys itself the moment they close the tab or log out. This zero-footprint web pattern protects your data assets even if a clinician’s physical laptop is lost or compromised.
Reality Check: What It Takes to Modernize
The true investment timeline and budget for a legacy replacement depend entirely on your data volume, the number of internal workflows, and the state of your existing databases.
Organizational Scale | Typical Transition Timeline | Typical Investment Budget |
Small Outpatient Clinic | 6 to 9 Months | $150,000 to $500,000 |
Multi-Site Specialty Practice | 9 to 12 Months | $500,000 to $1,500,000 |
Regional Provider Network | 12 to 18 Months | $1,000,000 to $5,000,000 |
Enterprise Hospital System | 12 to 24 Months | $2,000,000+ |
Operational Readiness: Are You Ready to Migrate?
Your technical steering committee can use this working matrix to check if your infrastructure is prepared for data extraction and system modernization.
Target Area | Core Operational Requirement | Ready? (Yes/No) |
Data Inventory | We have mapped every historical patient record and data silo across facilities. | |
Quality Audit | We ran an initial data quality assessment to identify corrupted or empty fields. | |
Interoperability | Our target database schemas are designed around native FHIR api web services. | |
Archive Policy | A strict, legally compliant data preservation retention policy has been approved. | |
Integration Map | Every required laboratory, pharmacy, and payer API integration is fully documented. | |
Access Control | Logins require Multi-Factor Authentication and strict role-based data isolation. | |
Session Security | Communication uses a Zero-Footprint pattern to disable local device data caching. | |
Failover Procedures | Step-by-step rollback paths are fully documented for every phase of rollout. |
Connected Ecosystem Insights
Building a reliable, fast clinical platform requires matching great database engineering with scalable communication channels and smart user psychology.
- Integrating Virtual Care Natively: Adding real-time telehealth options directly into your custom platform requires a highly scalable, low-latency infrastructure design. Review our framework: Emerline Telehealth Development Roadmap.
- Minimizing Cloud Overhead Costs: Discover how custom interface engineering and self-service modules reduce long-term operating expenses: How a User-Friendly App Reduces Healthcare Costs.
Frequently Asked Questions
1. Should we migrate all historical patient data into our new system?
Practically speaking, no. Moving decades of messy, unvalidated data into your new platform slows down performance and complicates development. The cleanest strategy is to migrate active clinical data from the last three years into the new platform, while routing the rest into a secure, low-cost read-only cold archive for compliance audits.
2. How do we prevent duplicate data entry while running two systems at once?
We use real-time integration middleware. When a doctor or administrative staff member updates a patient chart or logs an appointment on one platform, the middleware instantly captures that event and replicates the data change across the parallel core, keeping both platforms synchronized automatically.
3. Can our clinicians access web-native health portals safely on mobile devices?
Yes, provided you implement the right security architecture. Mobile browser security relies on entirely disabling local data storage on the phone, utilizing biometric validation via WebAuthn protocols, and enforcing aggressive session expiration windows.
4. What are the actual risks of a failed or incomplete data preservation audit?
The consequences are severe. Violating health data retention laws can land you with millions of dollars in regulatory fines, immediate loss of your processing licenses from health authorities, complex legal lawsuits, and a permanent blow to market trust.
5. How does a modern system verify insurance eligibility automatically?
The backend uses automated Electronic Data Interchange transactions to ping insurance databases through secure web connections the moment a patient books a slot. Within seconds, the portal reads the response and updates the screen with exact copay details, completely eliminating manual verification calls.
Summary: Focus on Data Agility
Replacing a legacy EHR platform is never just a technology project. It is a data governance initiative, an operational transition, and one of the most important infrastructure decisions your organization will make in a decade.
The teams that succeed are those that avoid aggressive, single-day cutovers, prioritize open data interoperability from day one, and treat historical record preservation as a core strategic requirement. Building a flexible, decoupled, cloud-native data engine today ensures your healthcare network is perfectly positioned to scale alongside the next generation of connected care.
| SUCCESS ARCHITECTURE BLUEPRINT | |
| Migration Pattern | Progressive Sidecar Model |
| Integration Model | Asynchronous Event Bus |
| Data Integrity | Automated Cleansing & ETL |
The long-term value of an EHR upgrade project depends entirely on architectural flexibility. Organizations that prioritize native interoperability, event-driven microservices, and zero-trust security today will own the next generation of digital healthcare delivery.
Disclaimer & Limitation of Liability: The market projections, regulatory updates, and technical metrics presented in this guide are based on industry evaluations and analytical forecasts for informational purposes only. They do not constitute formal technical, legal, or medical advice. Emerline assumes no liability or responsibility for any business decisions, implementation strategies, or third-party compliance outcomes resulting from the use of the information provided in this guide.
Published on Feb 1, 2026





